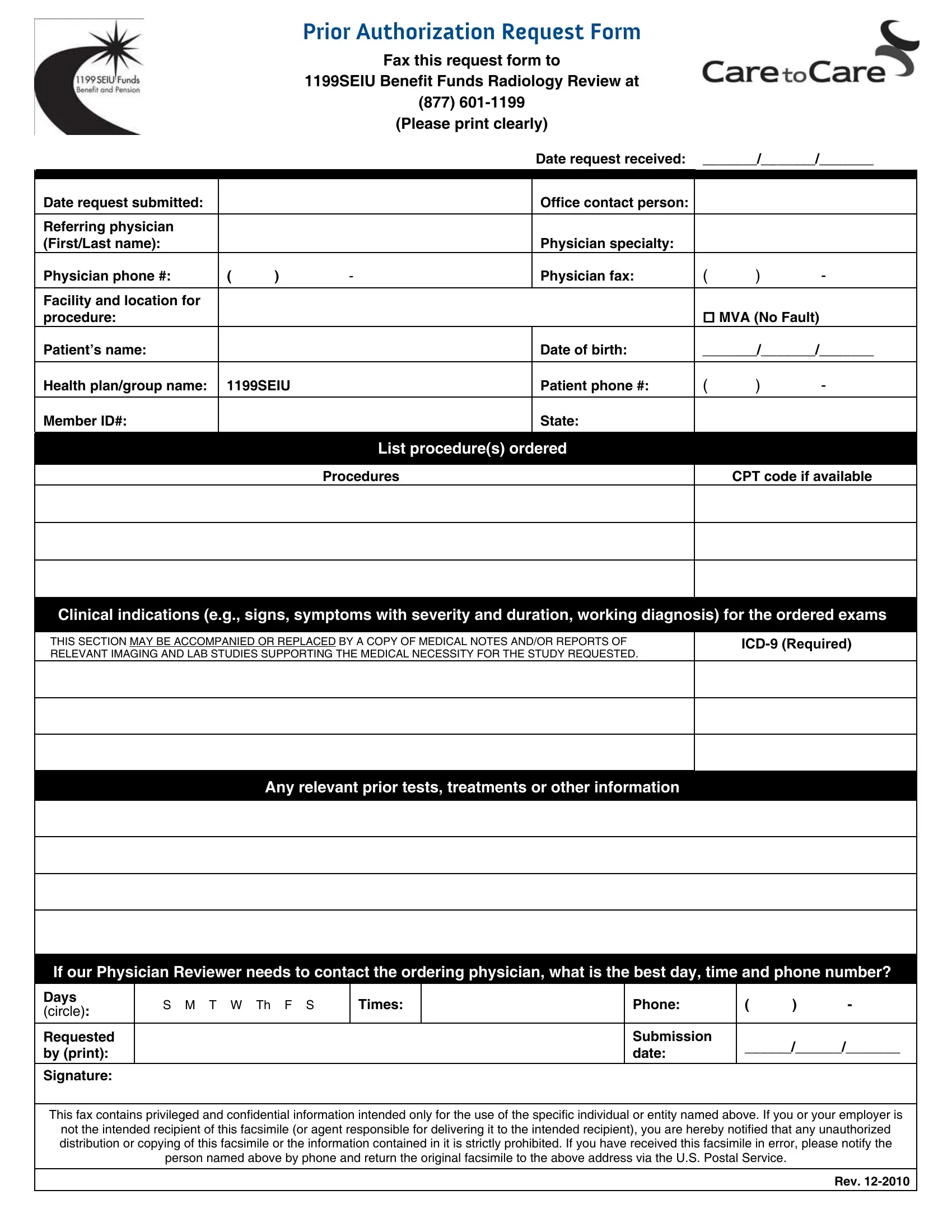
The 1199 Authorization Form represents a crucial document within the medical and healthcare industry, particularly for those involved with the 1199SEIU Benefit Funds. This specific form is designed to streamline the process of requesting radiology reviews by providing a structured way for healthcare providers to submit necessary information. The form requires comprehensive details such as the date of the request, contact information for the office and referring physician, the patient's details including their name, date of birth, and member ID, alongside the health plan or group name. It notably includes sections for specifying the procedures requested with their respective CPT codes, clinical indications for the exams, and any relevant prior tests or information that supports the medical necessity of the study requested. The form also prompts for preferred contact times for the ordering physician, in case the physician reviewer needs further consultation. Processing this form involves faxing it to a designated number, ensuring that sensitive patient information is handled securely and efficiently. The stipulated guidelines and the declaration that the fax contains privileged and confidential information underline the importance of meticulous handling and the privacy considerations integral to the use of the 1199 Authorization Form. The acknowledgment of receipt by unauthorized personnel and the prompt direction to return the document to the sender further accentuates the protective measures in place for patient data.
| Question | Answer |
|---|---|
| Form Name | 1199 Authorization Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | ICD-9, severity, CPT, IMAGING |
Prior Authorization Request Form
Fax this request form to
1199SEIU Benefit Funds Radiology Review at
(877)
(Please print clearly)
|
|
|
|
Date request received: |
_______/_______/_______ |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date request submitted: |
|
|
|
Office contact person: |
|
|
|
|
|
|
|
|
|
|
|
Referring physician |
|
|
|
|
|
|
|
(First/Last name): |
|
|
|
Physician specialty: |
|
|
|
Physician phone #: |
( |
) |
- |
Physician fax: |
( |
) |
- |
|
|
|
|
|
|
|
|
Facility and location for |
|
|
|
|
|
|
|
procedure: |
|
|
|
|
MVA (No Fault) |
|
|
Patient’s name: |
|
|
|
Date of birth: |
_______/_______/_______ |
||
|
|
|
|
|
|
|
|
Health plan/group name: |
1199SEIU |
|
Patient phone #: |
( |
) |
- |
|
Member ID#:
State:
List procedure(s) ordered
Procedures
CPT code if available
Clinical indications (e.g., signs, symptoms with severity and duration, working diagnosis) for the ordered exams
THIS SECTION MAY BE ACCOMPANIED OR REPLACED BY A COPY OF MEDICAL NOTES AND/OR REPORTS OF RELEVANT IMAGING AND LAB STUDIES SUPPORTING THE MEDICAL NECESSITY FOR THE STUDY REQUESTED.
Any relevant prior tests, treatments or other information
If our Physician Reviewer needs to contact the ordering physician, what is the best day, time and phone number?
Days |
S M T W Th F S |
Times: |
|
Phone: |
( |
) |
- |
(circle): |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Requested |
|
|
|
Submission |
______/______/_______ |
||
by (print): |
|
|
|
date: |
|||
|
|
|
|
|
|
||
Signature:
This fax contains privileged and confidential information intended only for the use of the specific individual or entity named above. If you or your employer is
not the intended recipient of this facsimile (or agent responsible for delivering it to the intended recipient), you are hereby notified that any unauthorized distribution or copying of this facsimile or the information contained in it is strictly prohibited. If you have received this facsimile in error, please notify the person named above by phone and return the original facsimile to the above address via the U.S. Postal Service.
Rev.