
It is possible to work with 1199 seui benefits fund disabilty forms effortlessly with the help of our online PDF editor. To have our editor on the leading edge of convenience, we strive to put into practice user-driven features and improvements regularly. We're routinely pleased to receive feedback - assist us with revolutionizing how we work with PDF files. If you're looking to get started, here is what you will need to do:
Step 1: Open the PDF form inside our editor by clicking the "Get Form Button" in the top section of this webpage.
Step 2: This editor provides the capability to work with PDF files in a variety of ways. Enhance it with your own text, adjust what's originally in the document, and place in a signature - all readily available!
It's an easy task to complete the document with our detailed guide! Here's what you have to do:
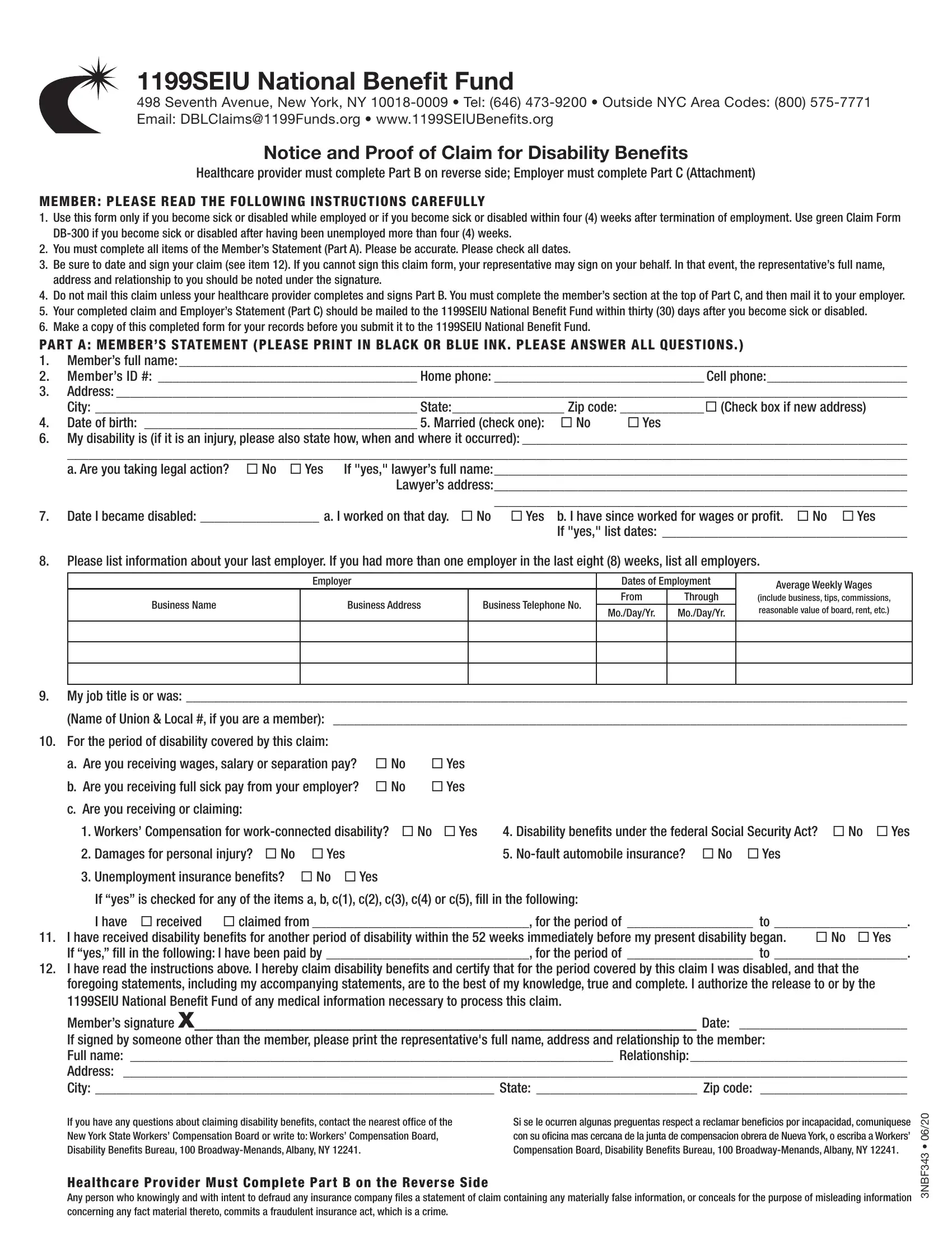
1. You need to fill out the 1199 seui benefits fund disabilty forms accurately, so take care while filling out the sections including these blanks:
2. Right after the last array of blank fields is completed, go to enter the applicable information in all these: For the period of disability, a Are you receiving wages salary, c Are you receiving or claiming, Workers Compensation for, Disability benefits under the, If yes is checked for any of the, I have received disability benefits, No Yes, If you have any questions about, Si se le ocurren algunas, and F B N .
It is easy to make an error while completing the If you have any questions about, for that reason be sure you go through it again before you decide to send it in.
3. The next part is considered fairly straightforward, The healthcare providers statement, Members full name Age Sex , Caesarean section, Was member hospitalized No Yes, c Treatment date If pregnancy, Was surgery performed No Yes, Enter dates for the following, a Date of your first treatment for, b Date of your most recent, c Date member was unable to work, d Date member will be able to, Month, Day, Year, and Even if considerable questions - each one of these form fields is required to be filled in here.
4. To go ahead, the next form section requires typing in several fields. Examples include In your opinion is this disability, Report of Services, Date of Service, Place of Service, Description of Service Rendered, Procedure ICD, CPT, Charge, Authorization to pay benefits to, Total , and F B N , which you'll find integral to carrying on with this PDF.
5. When you near the completion of this file, there are a few extra things to complete. Mainly, Member Please complete the, Date , Members full name , Members ID , Date disability began , DISCLOSURE OF INFORMATION The, HIPAA NOTICE In order to, ATTENTION PAYROLL DEPARTMENT The, EMPLOYERS STATEMENT TO BE, Date employee was employed , Date employee last worked before, and a Full sick pay received not the should be filled in.
Step 3: Soon after looking through your entries, click "Done" and you're good to go! Join FormsPal now and instantly access 1199 seui benefits fund disabilty forms, available for download. Each modification you make is conveniently preserved , which enables you to edit the form later as needed. FormsPal is devoted to the confidentiality of our users; we make sure all personal information coming through our editor is kept protected.