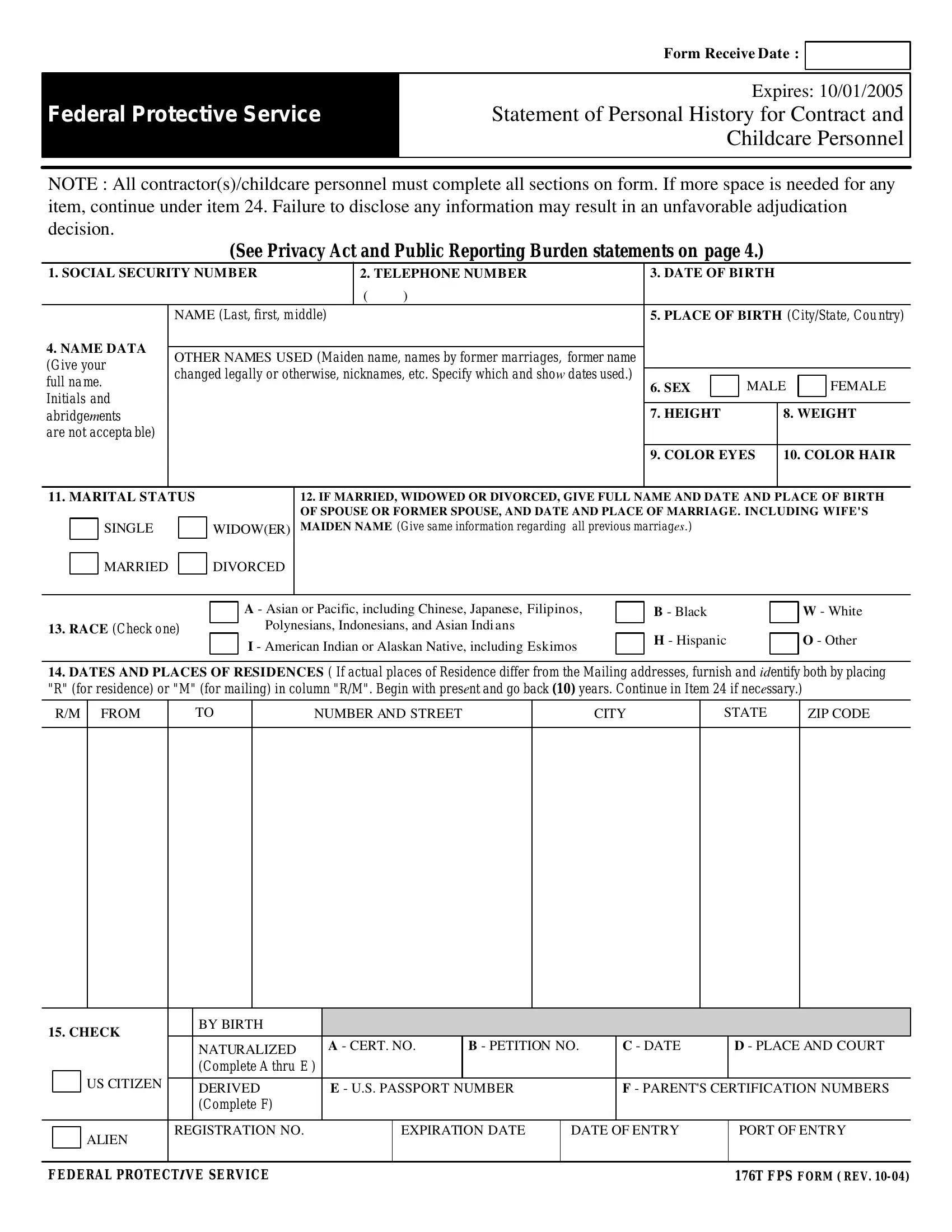
The 176T FPS form, issued by the Federal Protective Service and set to expire on October 1, 2005, represents a vital document required from all contractors and childcare personnel working under the auspices of the federal government. Designed to gather comprehensive personal histories, this form delves into various spheres of an applicant's background, including but not limited to social security numbers, employment history, education, and any legal infractions, with an explicit emphasis on ensuring the security and integrity of the federal workplace and those it serves. Applicants are urged to provide detailed responses for each section, and if the predefined space is insufficient, continuations are allowed under item number 24 to ensure completeness. A failure to disclose pertinent information, or the provision of false statements, is not taken lightly and could lead to significant legal ramifications, underscoring the form’s role in safeguarding the workplace against potential vulnerabilities that could compromise public safety and national security. The inclusion of a Privacy Act and Public Reporting Burden statement also highlights the federal government's commitment to transparency and the judicious use of applicants' personal information. Furthermore, the authorization section explicitly allows the Department of Homeland Security to access necessary records, ensuring that all data collected serves the purpose of a thorough and fair evaluation, encapsulating the form’s comprehensive approach towards maintaining a workforce that is both competent and trustworthy.
| Question | Answer |
|---|---|
| Form Name | 176T Fps Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | fps statement childcare sample, 176t statement history childcare, 176t form fill, fps 176t template |
|
FORM RECEIVE DATE : |
|
|
|
|
|
|
|
Federal Protective Service |
Expires: 10/01/2005 |
|
Statement of Personal History for Contract and |
||
|
Childcare Personnel |
|
|
|
|
|
|
|
NOTE : All contractor(s)/childcare personnel must complete all sections on form. If more space is needed for any item, continue under item 24. Failure to disclose any information may result in an unfavorable adjudication decision.
(See Privacy Act and Public Reporting Burden statements on page 4.)
1. SOCIAL SECURITY NUMBER |
|
2. TELEPHONE NUMBER |
3. DATE OF BIRTH |
|
|
|
||||||||
|
|
|
|
|
|
|
( |
) |
|
|
|
|
|
|
|
|
|
NAME (Last, first, middle) |
|
5. PLACE OF BIRTH (City/State, Cou ntry) |
|||||||||
4. NAME DATA |
|
|
|
|
|
|
|
|
|
|
|
|
||
OTHER NAMES USED (Maiden name, names by former marriages, former name |
|
|
|
|
|
|
||||||||
(Give your |
|
|
|
|
|
|
||||||||
changed legally or otherwise, nicknames, etc. Specify which and shoW dates used.) |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|||||||||
full name. |
6. SEX |
|
MALE |
|
FEMALE |
|||||||||
|
|
|
|
|
|
|
|
|||||||
Initials and |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
abridgeMents |
|
|
|
|
|
|
7. HEIGHT |
|
8. WEIGHT |
|||||
are not accepta ble) |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9. COLOR EYES |
10. COLOR HAIR |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. MARITAL STATUS |
12. IF MARRIED, WIDOWED OR DIVORCED, GIVE FULL NAME AND DATE AND PLACE OF BIRTH |
|||||||||||||
|
|
|
|
|
|
OF SPOUSE OR FORMER SPOUSE, AND DATE AND PLACE OF MARRIAGE. INCLUDING WIFE'S |
||||||||
|
|
SINGLE |
|
|
WIDOW(ER) |
MAIDEN NAME (Give same information regarding all previous marriagES.) |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
MARRIED
DIVORCED
13.RACE (Check one)
A - Asian or Pacific, including Chinese, Japanese, Filipinos, Polynesians, Indonesians, and Asian Indi ans
I - American Indian or Alaskan Native, includINg Eskimos
B - Black
H - Hispanic
W - White
O - Other
14.DATES AND PLACES OF RESIDENCES ( If actual places of Residence differ from the Mailing addresses, furnish and IDentify both by placing "R" (for residence) or "M" (for mailing) in column "R/M". Begin with presEnt and go back (10) years. Continue in Item 24 if necEssary.)
R/M
FROM
TO
NUMBER AND STREET
CITY
STATE
ZIP CODE
15. CHECK |
|
|
BY BIRTH |
|
|
|
|
|
|
||
|
|
|
|
|
NATURALIZED |
A - CERT. NO. |
B - PETITION NO. |
C - DATE |
D - PLACE AND COURT |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
US CITIZEN |
|
(Complete A thru E ) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
DERIVED |
E - U.S. PASSPORT NUMBER |
|
F - PARENT'S CERTIFICATION NUMBERS |
|||||
|
|
|
|
|
|
||||||
|
|
|
|
|
(Complete F) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ALIEN |
REGISTRATION NO. |
|
EXPIRATION DATE |
DATE OF ENTRY |
PORT OF ENTRY |
||||
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
FEDERAL PROTECTIVE SERVICE |
|
|
|
|
|
176T FPS FORM ( REV. |
|||||
16.EDUCATION ( All schools above elemeNtary )
NAME OF SCHOOL
ADDRESS
CITY
STATE
YEAR FROM YEAR TO
DEGREES
17.EMPLOYMENT ( List employment dates starting with your present employment for The last ten (10) years. Show ALL dates and addreSses when unemployed. Give name under which employed if different from nAme now used. )
FROM
TO
NAME OF EMPLOYER ( Firm or Agency) AND NAME OF SUPERVISOR
PHONE NUMBER
TYPE OF WORK
ADDRESS
CITY
STATE
REASON FOR LEAVING
18.HAVE YOU EVER BEEN DISMISSED OR FORCED TO RESIGN FROM ANY POSITION FOR CAUSE ?
YES
NO ( If answer is "YES" furnish details in Item 22 )
18a. MILITARY SERVICE
(Past to Present)
HAVE YOU EVER BEEN IN VIOLATION OF MILITARY OFFENSE OF COURT MARTIAL OR DISCHARGED FROM THE ARMED FORCES UNDER OTHER THAN HONORABLE CONDITIONS ?
|
|
YES |
|
NO ( If answer is "YES" furnish details in Item 22 ) |
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SERIAL NO. ( If none, give |
|
BRANCH OF SERVICE |
|
YEAR FROM |
YEAR TO |
|||
grade or rating at sepaRation.) |
|
( Army, Navy, Air Force, |
ETC.) |
|||||
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
19.HAVE YOU EVER BEEN ARRESTED, CHARGED, OR HELD BY FEDERAL, STATE, OR OTHER LAW ENFORCEMENT AUTHORITIES FOR ANY VIOLATION OF ANY FEDERAL LAW, MILITARY LAW, STATE LAW, COUNTY LAW, MUNICIPLE LAW, RE GULATIONS, OR ORDINANCE ? ( Do not include traffic violations for which a fine of $25 or less was imposed. All other charges must be included even If they were dismissed.)
YES
NO ( If answer is "YES" give full details below )
REASON CHARGED OR HELD
DATE
PLACE WHERE CHARGED OR HELD
DISPOSITION
FEDERAL PROTECTIVE SERVICE |
176T FPS FORM ( REV. |

19a. HAVE YOU EVER BEEN CHARGED, ARRESTED OR HELD BY ANY LOCAL, STATE, OR FEDERAL LAW ENFORCEMENT AGENCY FOR ANY VIOLATION OR OFFENSE INVOLVING: CHECK YES/NO AS TO ARREST. FAILURE TO PROVIDE ARREST INFORMATION MAY RESULT IN AN UNFAVORABLE ADJUDICATION DECISION.
|
|
Child |
|
|
|
|
|
Yes |
|
|
|
|
|
No |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
Sexual offender/registry |
|
|
|
|
|
Yes |
|
|
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Domestic Violence |
|
|
|
|
|
Yes |
|
|
|
No |
|
||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
REASON CHARGED OR HELD |
|
|
DATE |
|
|
PLACE WHERE CHARGED OR HELD |
DISPOSITION |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
20.RELATIVES ( Parents, spouse, divorced spouse, children, brothers, and sisters, living or dead. Name of spousE should include maiden name and any other names by previous marriage. If person is deceased, so state under "Address" and enter otHEr information at time of death. )
RELATION
NAME IN FULL
PHONE NUMBER
YEAR OF BIRTH
ADDRESS
CITY
STATE
COUNTRY OF BIRTH
PRESENT CITIZENSHIP
21. REFERENCES ( Name three persons, not relatives or employers, who are well acquainted WIth you. )
NAME
ADDRESS
CITY
STATE
YEARS KNOWN
FEDERAL PROTECTIVE SERVICE |
176T FPS FORM ( REV. |
22.SPACE FOR CONTINUING ANSWERS TO OTHER QUESTIONS ( Show item numbers to which answers apply. Attach a separate sheet if tHEre is not enough space heRe. )
I hereby authorize the Department of Homeland Security to obtain any information required from the Federal goveRNment and/or state agencies, including but not limited to, the Federal Bureau of Investigation (FBI), the Defense InvESTIgation Service (DIS), the U.S. Office of Personnel Management (OPM), the Department of Homeland Security (DHS), (if applicable), and from the State Criminial History Repository (Childcare employees only) of each state where I have resided.
23.I have been notified of any employer's obligation to require a criminal history records check as a condition of employment and of my
AUTHORI- |
right to obtain a copy of the criminal history report by writing to the Department of Homeland Security, Freedom of Information |
|
ZATION |
Officer. I understand that I have a right to challenge the accuracy and competencies of any information contained in the report. I also |
|
AND |
||
understand that this information will be treated as privileged and confidential information. Case files are handled under the procedures |
||
RELEASE |
||
for safeguarding records. |
||
|
||
|
I release any individual, including records custodians, any component of the U.S. Government or the individual State Criminal History |
|
|
Repository supplying information, from all liability for damages that may result on account of compliance or any ATtempts to comply |
|
|
with this authorization. This release is binding, now and in the future, on my heirs, assigns, associates, and personal represenTative(s) |
|
|
of any nature. Copies of this authorization that show my signature are as valid as the original release signed by me. |
Privacy Act of 1974 compliance information. Solicitation of information contained herein in authorized by ExecUtive Order 10450, and/or Section 231 of the Crime Control Act of 1990 (42 U.S.C. 13041), and may be used as a basis for suitability deTErminations. Your social security number is being requested pursuant to Executive Order 9397. Disclosure of the information by you is voluntary.
24.PRIVACY Information may be transferred as a routine use to appropriate federal, state, local, or foreign agencies when relevant to civil, criminal
ACT OF 1974 |
or regulatory investigation, prosecutions, or pursuant to a request by DHS or such other agency is in connection with the hiring or |
|||
COMPLI - |
retention of an employee, the issuance of a license, grant, or other benefit. Information also may be transferred as a routine use to a |
|||
ANCE IN - |
||||
duly authorized official engaged in aN investigation or settlement of a grievance, complaint, or appeal filed by an employee. Failure to |
||||
FORMATION |
||||
provide information requested on this form may result in the government's inability to determine your suitABility for the position |
||||
|
applied for or occupied, and may affect your prospects for employment or continued employment under a government coNtract, or at a |
|||
|
federal facility, or with a governmeNT license. |
|
|
|
|
|
|||
25. PUBLIC |
Public reporting burden for this collection of information is estimated to average 8 hours per response, including the time for |
|||
REPORTING |
reviewing instructions, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the |
|||
BURDEN |
collection of information. Send comments regarding this burden estimate or any other aspects of this collection of information, |
|||
STATEMENT |
including suggestions for reducing this burden, to Security Division (PSS), Office of Federal PROtective Service, Washington, DC |
|||
|
20405; and to the Office of Management and Budget, Paperwork Reduction Project |
|||
|
|
|
|
|
|
FALSE STATEMENTS ARE PUNISHABLE BY LAW AND COULD |
Before signing this form, review it carefully tO make sure |
||
26. |
RESULT IN FINES AND/OR IMPRISONMENT UP TO FIVE YEARS. |
you have answered all questions fully and correctly. |
||
CERTIFI- |
|
|
|
|
|
SIGNATURE |
DATE |
||
CATION |
I declare under penalty of perjury that the statements made by |
|||
|
|
|||
|
|
|
||
|
me on this form are true, complete and correct. |
|
|
|
|
|
|
|
|
FEDERAL PROTECTIVE SERVICE |
176T FPS FORM ( REV. |
* This is a temporary form expires 10/1/05.