
To fill out the 470 4339 form online, you do not need to download any application. Use our free PDF editor directly in your browser. Our tool is designed to make the process as straightforward as possible for executors and family members handling Iowa estate recovery paperwork.
Step 1: Click the orange "Get Form" button above. This opens our PDF tool so you can begin completing the form right away.
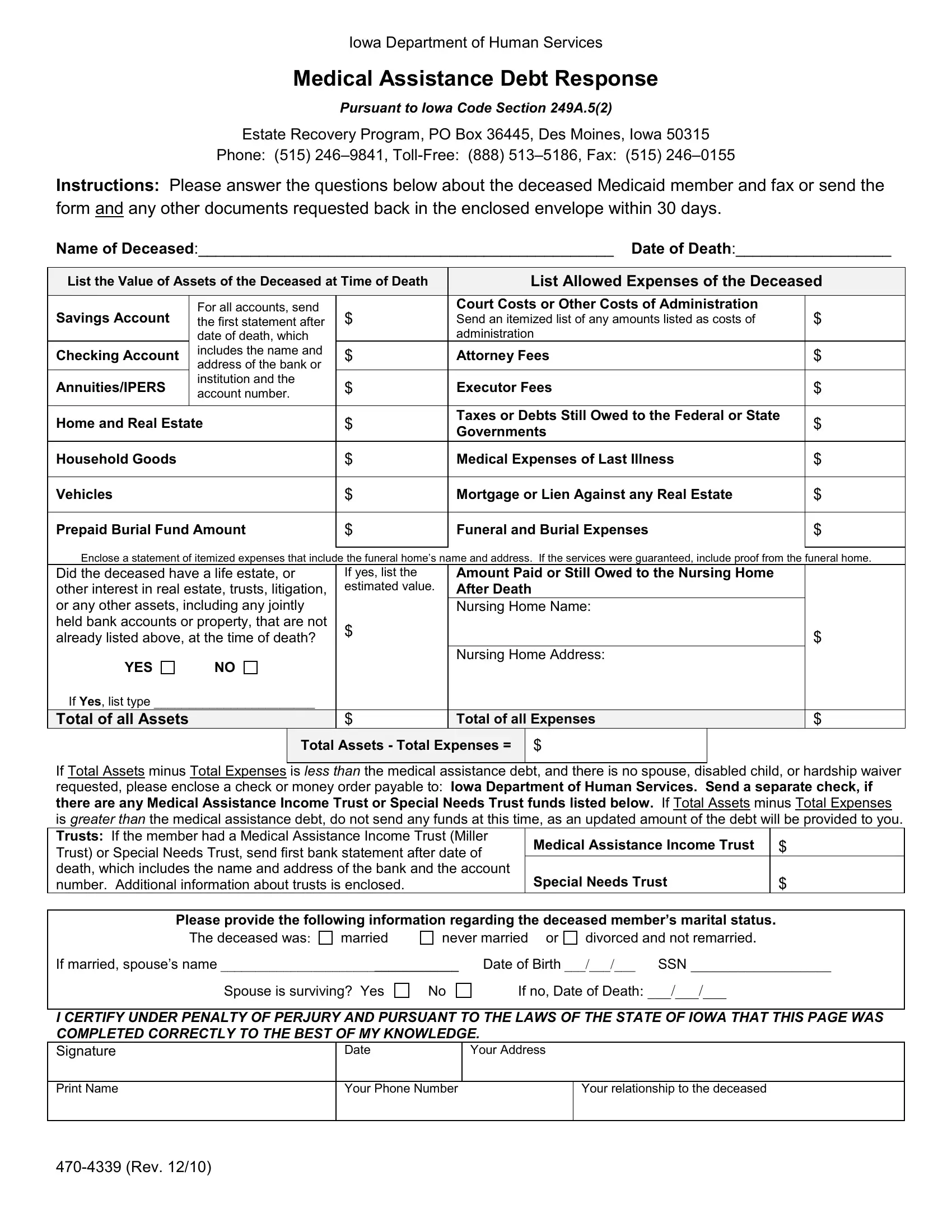
Step 2: Use our PDF editor to fill in all required fields. You will need to provide information about the deceased's assets and any debts or expenses. The main fields include:
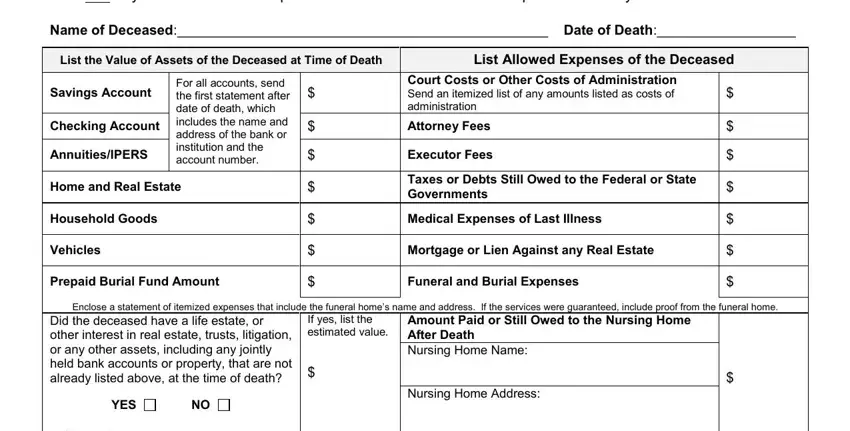
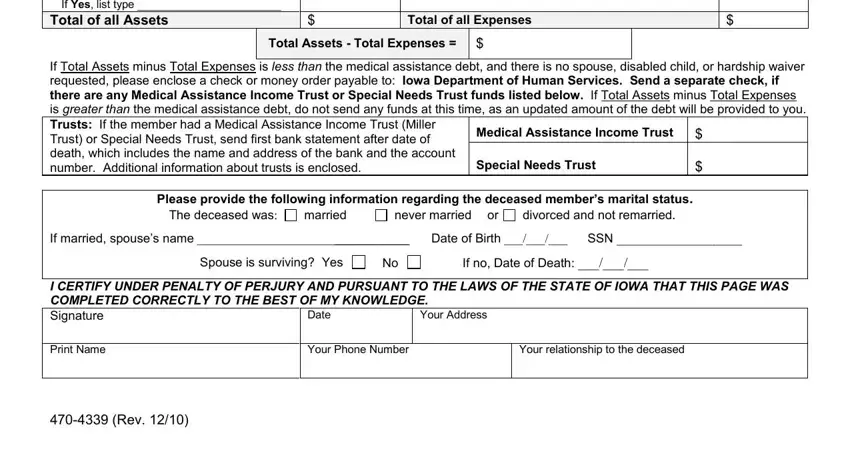
Step 3: Fill in all the required sections, including asset types, total assets, total expenses, and information about the deceased's marital status. Key fields to complete are: type of assets, total of all assets, total of all expenses, net estate value, medical assistance income trust details, and the deceased's personal information.
Step 4: Review all entries carefully before finalizing. Once done, click "Done" to save. With a FormsPal account, you can download the completed 470 4339 form as a PDF or send it via email. Your data is protected with secure encryption and is never shared or stored without your consent.