
When working in the online PDF editor by FormsPal, you'll be able to complete or alter 11th right here and now. To retain our editor on the cutting edge of practicality, we strive to put into practice user-oriented features and enhancements on a regular basis. We are at all times grateful for any suggestions - join us in revolutionizing PDF editing. Here is what you would have to do to begin:
Step 1: Click the "Get Form" button above. It'll open up our pdf editor so you can start filling in your form.
Step 2: The tool offers the opportunity to customize PDF documents in many different ways. Modify it by writing customized text, adjust what's already in the document, and include a signature - all at your fingertips!
In an effort to finalize this PDF document, make sure that you provide the required information in every single area:
1. It's very important to fill out the 11th properly, therefore take care when filling in the segments containing these particular blank fields:
2. Once your current task is complete, take the next step – fill out all of these fields - Insurers representative, Telephone number, Insurer claim or file number, If bringing arbitration against, MVAIC claim number , and Did the accident occur in New York with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
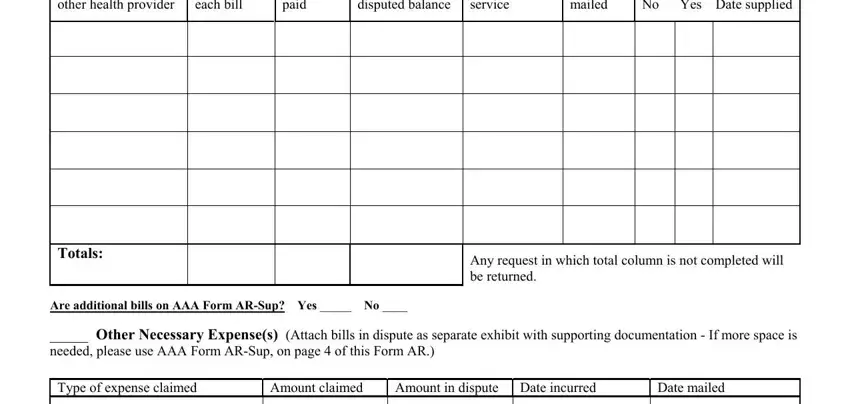
3. This next section will be focused on Part Requests for Special, Doctor hospital or other health, Amount of each bill, Amount paid, Unpaid or disputed balance, Dates of service, Date bill mailed, and Was verification requested No Yes - fill in all these empty form fields.
Be extremely attentive when filling in Unpaid or disputed balance and Doctor hospital or other health, because this is the section where a lot of people make errors.
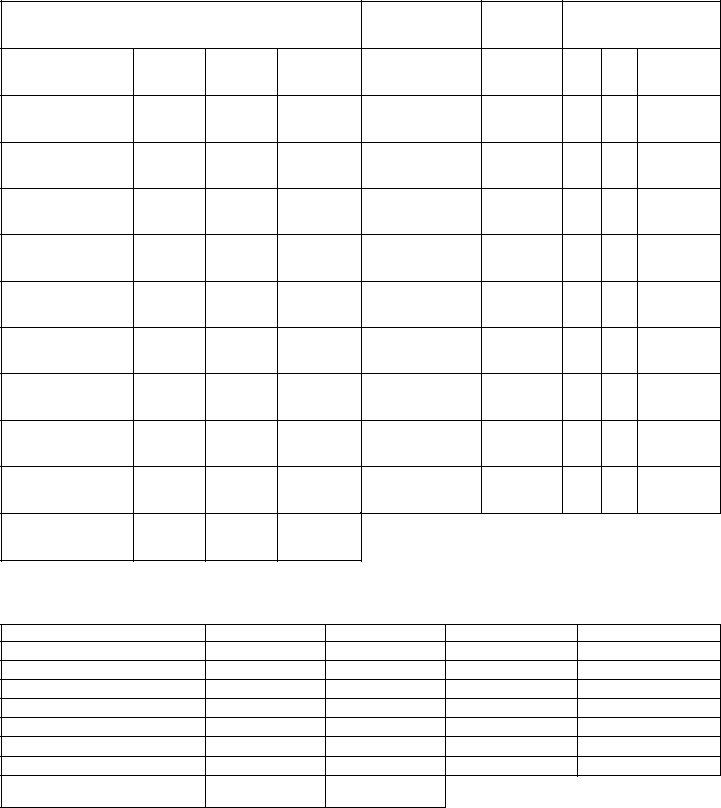
4. Filling out Doctor hospital or other health, Amount of each bill, Amount paid, Unpaid or disputed balance, Dates of service, Date bill mailed, Was verification requested No Yes, Totals, Any request in which total column, Are additional bills on AAA Form, Type of expense claimed, Amount claimed, Amount in dispute Date incurred, Any request in which total column, and Date mailed is essential in this fourth stage - make certain that you take your time and take a close look at every blank!
5. This last stage to finalize this document is critical. You must fill out the required fields, such as Type of expense claimed, Totals, Amount claimed, Amount in dispute Date incurred, Any request in which total column, Date mailed, and Are additional expenses on AAA, before submitting. Or else, it may end up in an incomplete and possibly incorrect form!
Step 3: Before finishing the document, it's a good idea to ensure that blank fields have been filled out the correct way. When you believe it is all fine, click “Done." Create a free trial plan with us and gain immediate access to 11th - which you'll be able to then work with as you want inside your FormsPal cabinet. At FormsPal, we strive to make sure that all your information is stored protected.