An employee accident report is a crucial document used to record and communicate the details of workplace accidents, whether minor or severe, which can significantly impact employees’ health and well-being. Organizations must thoroughly investigate these incidents to ensure the safety of their workforce and, in some cases, to satisfy legal requirements. The primary step in this process is providing prompt and appropriate medical care for the affected individual.
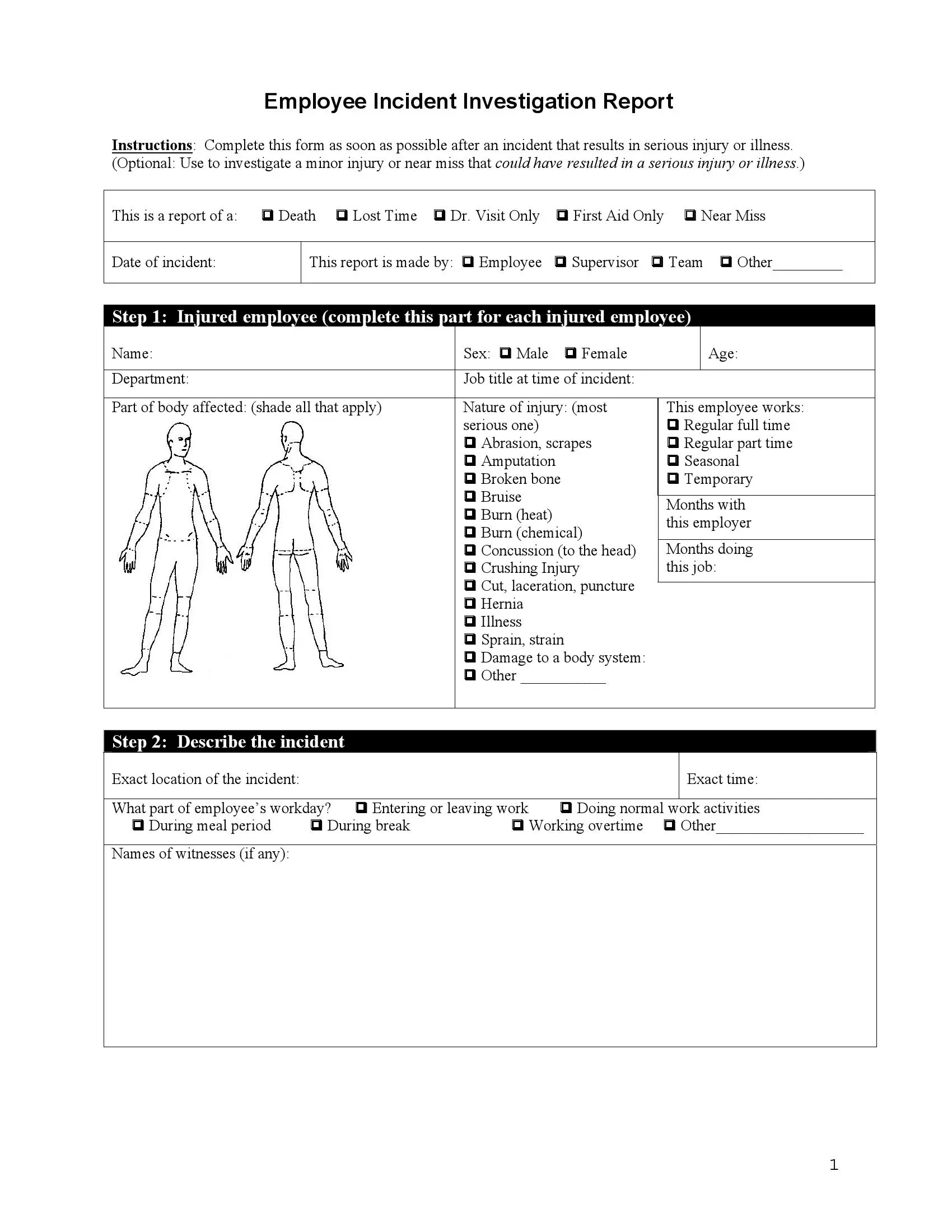
The Employee Incident Report Form serves as a vital tool for employees, coworkers, and supervisors to document the incident. This three-page document streamlines the investigation process by offering a structured format to record essential information.
Designed to accommodate a wide range of workplace accidents, this versatile template can be used to report severe injuries (such as amputations, concussions, or burns) as well as minor incidents that may result in future health issues or discomfort. By using the Workplace Accident Report Form, companies can foster a safer work environment and take necessary steps to prevent similar occurrences in the future.
The U.S. Department of Labor (DOL) plays a significant role in workplace safety and incident reporting through its various agencies, particularly the Occupational Safety and Health Administration (OSHA), which is responsible for establishing and enforcing workplace safety standards and regulations in the United States.
Adhering to OSHA regulations and guidelines when reporting incidents helps organizations maintain compliance, protect their employees, and foster a safe work environment.
Step 1. Download the Template
Acquire the appropriate Employee Accident Report form using our form-building software, which allows you to download various legal templates in seconds.
Step 2. Review the Instructions
Read the instructions provided at the beginning of the form, outlining when it should be completed, and proceed to fill out the form.

Step 3. Identify the Reason for the Report
Select the relevant reason for submitting the report from the six available options in the provided chart.

Step 4. Record the Incident Date
Enter the date on which the incident took place.

Step 5. Indicate the Report’s Creator
Next to the date, you will see four options that say who is creating this report. Such templates can be signed by:
If none of these is relevant, you have the “other” line at the bottom in which you may specify who is reporting.

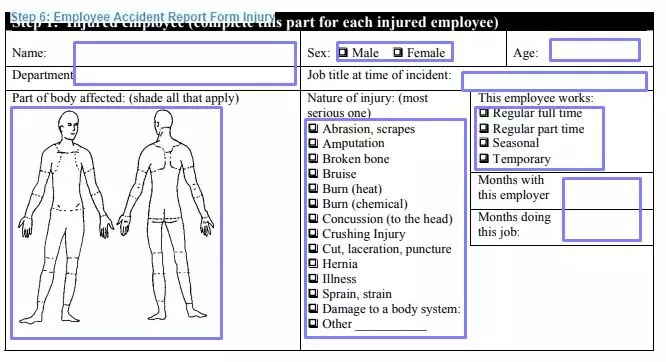
Step 6. Provide Employee and Injury Details
Complete the section with information about the injured employee and their injury, ensuring to fill out a separate form for each affected individual if multiple employees were injured.
Step 7. Describe the Incident
Provide a detailed account of the incident, addressing each question in the designated section and including any additional information as necessary.

Add the names of witnesses if there were any. If there are statements written by witnesses, the incident’s photos, or any other drawings (like maps), write the number of each in the designated position.


Answer if the employee used any personal protective equipment at the moment of the incident. Then, provide the full description of the events leading to the incident step by step, including the names of various tools, machines, and other essential objects that participated (if any). You may attach a sheet or two to the form if you need additional space.

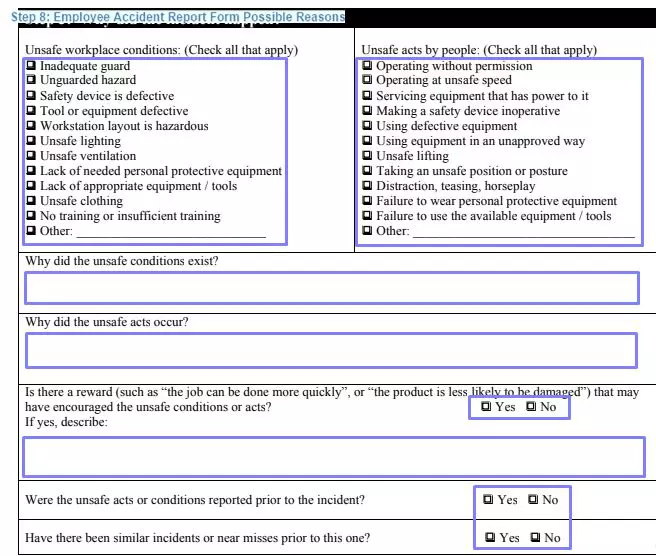
Step 8. Select Possible Causes for the Incident
Choose from the lists of unsafe working conditions and unsafe acts by people, explaining why the selected points may have contributed to the incident. Answer the subsequent “yes or no” questions related to the employee’s workplace.
Step 9. Submit Recommendations for Prevention
Choose from the ten provided options or suggest your own actions to prevent similar future incidents. Describe in detail how to implement the selected actions.

Step 10. Sign and Date the Report
After completing the form, sign and provide personal details, including your name, title, and department. Date the form. If applicable, have the investigation team members, reviewing supervisor, or human resources staff sign and date the “reviewed by” section.
Once the form is complete and reviewed, it will be forwarded to the investigation team to determine employee compensation and any necessary changes to working conditions.

Accuracy is crucial when completing an incident report because it ensures that the information provided accurately represents the events that transpired. Providing accurate information serves several essential purposes:
Collecting and including supporting documentation when filling out an incident report strengthens the report’s credibility and provides a more comprehensive understanding of the event. Supporting documentation may include:
By gathering and including relevant supporting documentation in the incident report, you can create a more robust and reliable account of the incident, assisting in the investigation process and the implementation of appropriate corrective actions.