
Whenever you wish to fill out ada health history form 2021, you won't have to install any applications - simply use our PDF tool. FormsPal team is committed to making sure you have the ideal experience with our tool by regularly introducing new functions and upgrades. Our editor has become much more intuitive with the newest updates! Now, editing PDF documents is a lot easier and faster than ever before. To start your journey, go through these basic steps:
Step 1: Open the form in our tool by clicking the "Get Form Button" in the top part of this webpage.
Step 2: As you start the tool, you will see the form made ready to be filled in. In addition to filling in various blank fields, you could also perform various other things with the PDF, specifically adding custom textual content, changing the original text, adding illustrations or photos, signing the document, and a lot more.
It really is simple to complete the form with this helpful guide! This is what you should do:
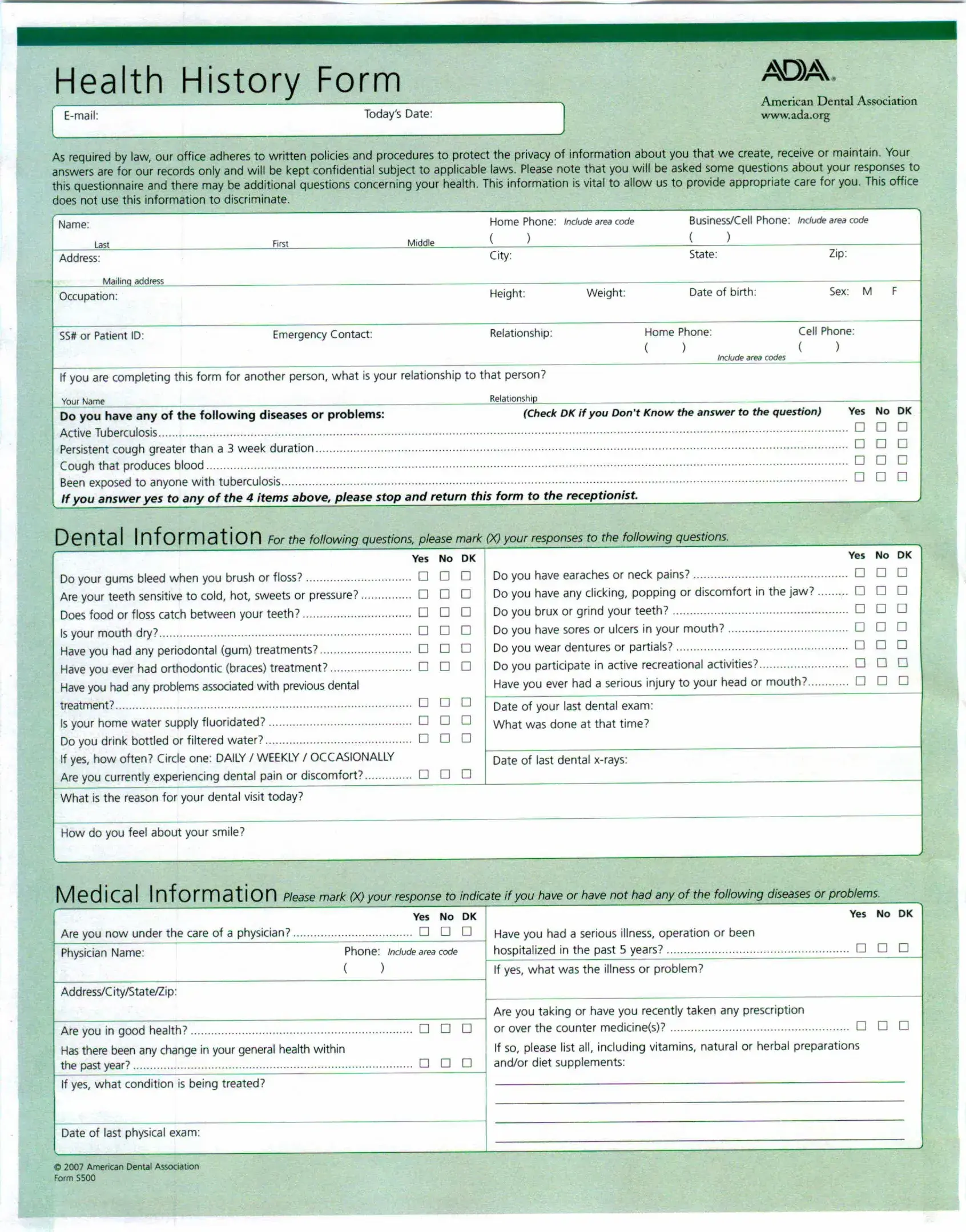
1. You should fill out the ada health history form 2021 correctly, thus take care when filling in the segments including these blanks:
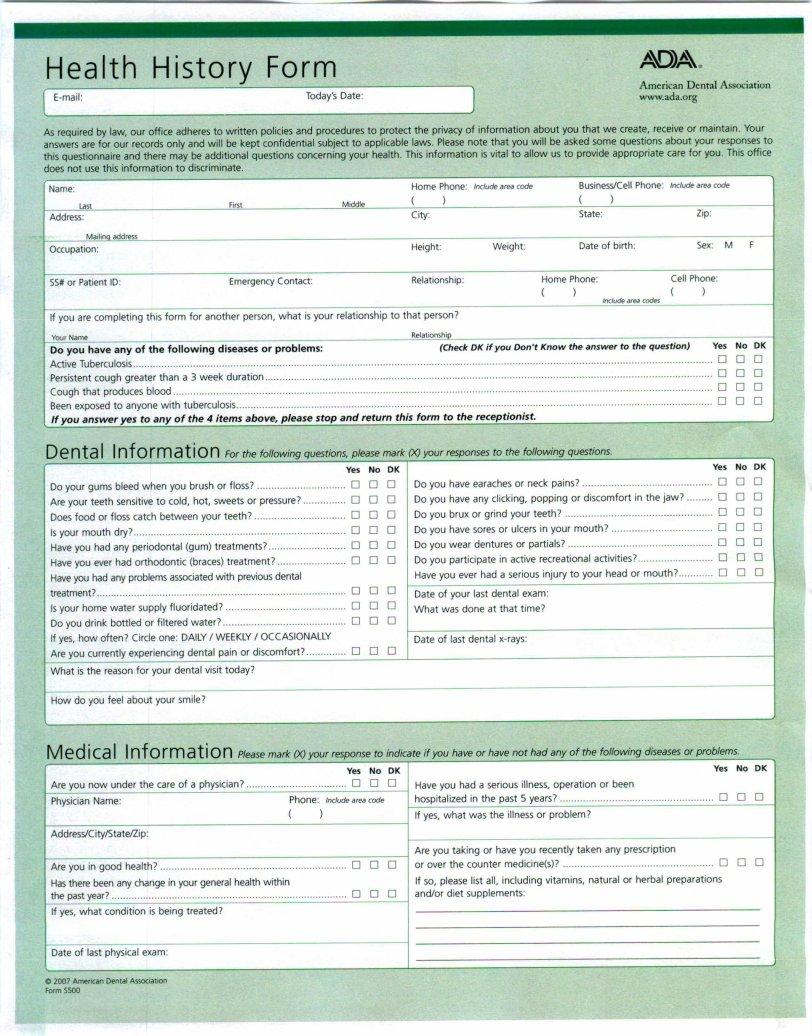
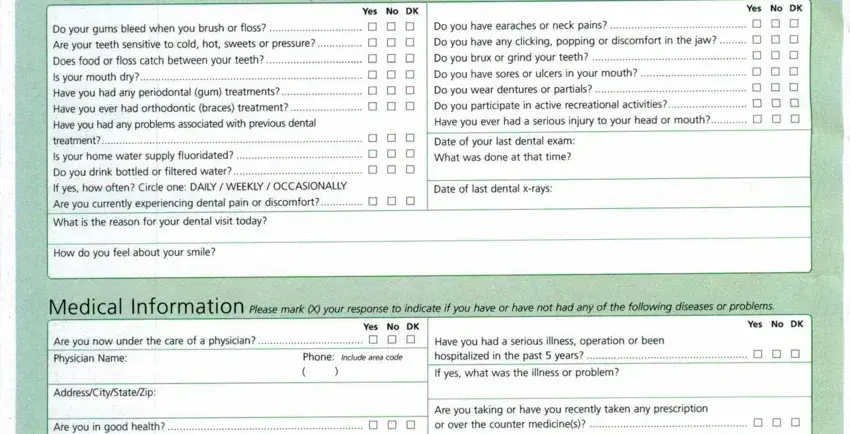
2. Your next part is to fill out the next few blanks: Den t a I Infor mat, ion For the following questions, Yes No OK, Yes No OK, Do your gums bleed when you brush, in the jaw Do you brux, gum treatments D D Do you wear, Do you have earaches or neck pains, Is your mouth dry, Do you have any clicking popping, Have you had any problems, treatment Is your home water, D D D Date of your last dental exam, time, and If yes how often Circle one DAILY.
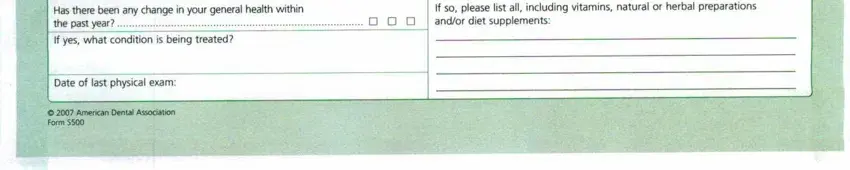
3. This third section should be quite easy, Hasthere been any change in your, If yes what condition is being, If so please list all including, D D D andor diet supplements, Date of last physical exam, C American Dental Association, and Form S - every one of these blanks has to be completed here.
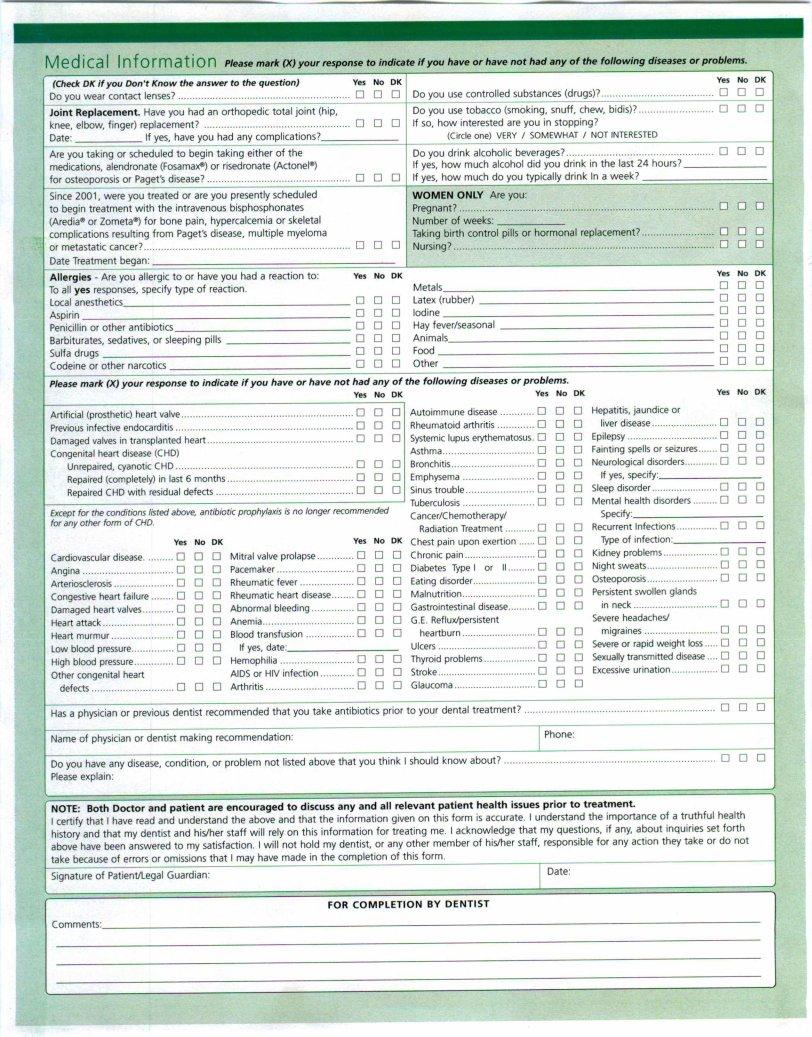
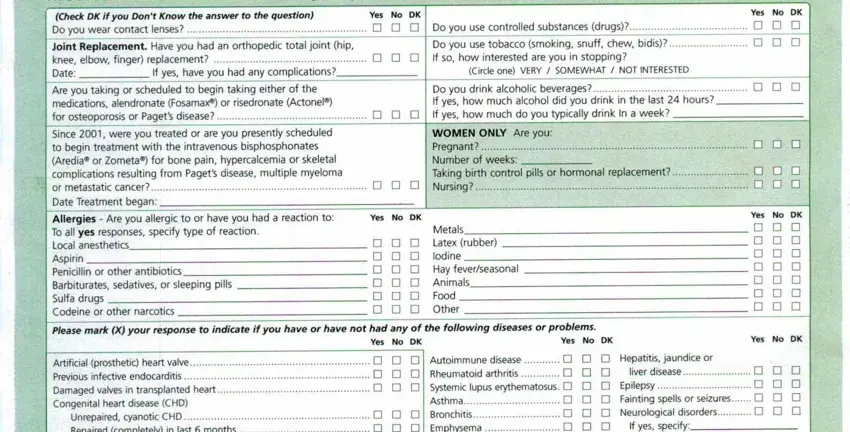
4. Completing Me die a I Infor mat ion Please, Check DK if you Dont Know the, to the question, Yes No OK, Do you use controlled substances, Joint Replacement Have you had an, If yes have you had any, hip, joint, Do you use tobacco smoking snuff, Circleone VERYI SOMEWHATI, Are you taking or scheduled to, Do you drink alcoholic beverages, Since were you treated or are you, and Date Treatment began is key in the next section - make sure to don't hurry and fill in each and every empty field!
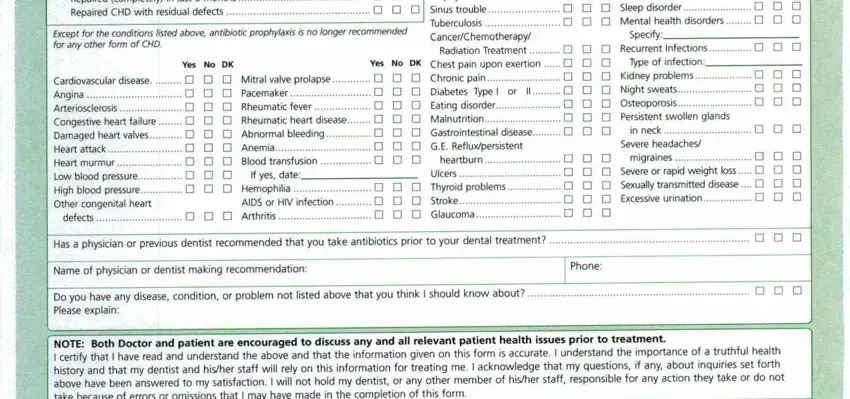
5. To wrap up your document, the particular part has some additional fields. Filling in Unrepaired cyanotic CHD, Except for the conditions listed, form of CHD, Autoimmune disease Rheumatoid, Yes No OK, Cardiovasculardisease Angina, Other congenital heart, defects, Mitral valve prolapse Pacemaker, If yes date, Radiation Treatment Yes No OK, heartburn Ulcers Thyroid, Hepatitis jaundice or liver, Specify, and Typeof infection should finalize the process and you will be done very quickly!
It is easy to make a mistake when filling in your form of CHD, thus you'll want to go through it again prior to deciding to finalize the form.
Step 3: Glance through all the details you've inserted in the blanks and press the "Done" button. Sign up with FormsPal today and instantly get ada health history form 2021, set for download. Every single edit made is conveniently saved , helping you to edit the pdf at a later time as needed. Here at FormsPal, we do our utmost to be certain that all your details are stored secure.