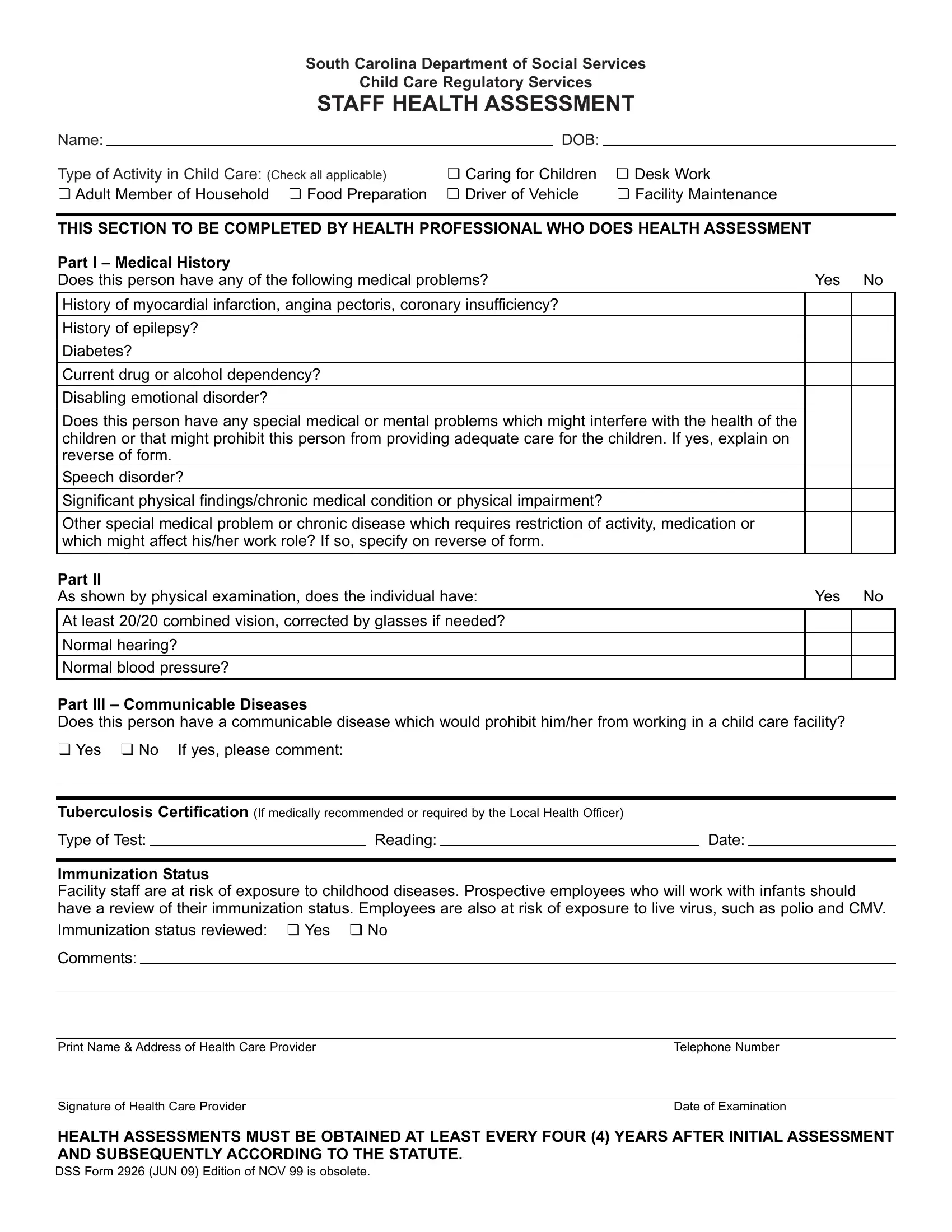
The DSS Health Assessment form, designed by the South Carolina Department of Social Services, specifically for Child Care Regulatory Services, plays a pivotal role in ensuring the well-being and safety of children in child care settings. This comprehensive form focuses on evaluating the health status of individuals involved in child care through various capacities, including direct care, food preparation, and maintenance, among others. It is structured to be filled out in parts, with the initial section capturing personal details and the kind of activities the individual will engage in at the child care facility. A significant portion is reserved for a health professional to complete, which covers a detailed medical history, physical examination findings, and an evaluation of communicable diseases, vital for preventing any potential health risks to children. Moreover, the form addresses the importance of candidates having a current review of their immunization status, given the high exposure risk to childhood illnesses within child care environments. Completing this form accurately and periodically, as mandated at least every four years, is crucial for maintaining a healthy and secure setting for children, staff, and household members involved in any child care services.
| Question | Answer |
|---|---|
| Form Name | Dss Health Assessment Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | dss form2926, form dss 2926 form, dss form 2926, form dss 2926 staff health assessment |
