
Making use of the online PDF editor by FormsPal, it is possible to complete or edit aetna practitioner and provider complaint and appeal form right here. We at FormsPal are committed to providing you the ideal experience with our editor by consistently releasing new capabilities and upgrades. With these improvements, using our editor gets better than ever! By taking some simple steps, you may begin your PDF editing:
Step 1: Access the form in our editor by clicking the "Get Form Button" in the top area of this page.
Step 2: The editor will let you modify your PDF form in a variety of ways. Transform it with your own text, adjust what's originally in the document, and put in a signature - all at your fingertips!
It is simple to fill out the document with this helpful tutorial! Here's what you should do:
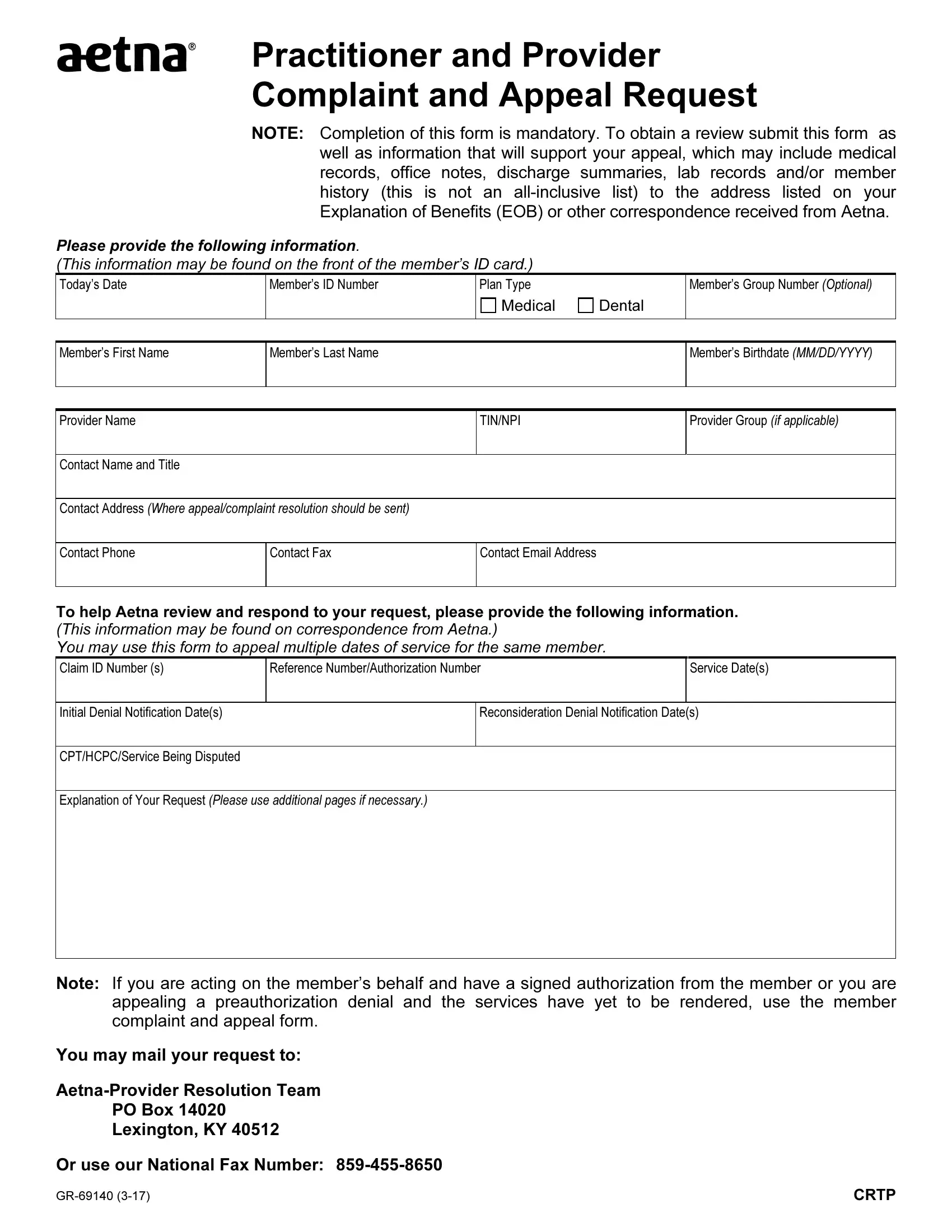
1. When filling out the aetna practitioner and provider complaint and appeal form, ensure to complete all of the needed blanks within the relevant form section. This will help to speed up the work, enabling your information to be handled promptly and accurately.
2. The subsequent stage is usually to fill out the following fields: Initial Denial Notification Dates, Reconsideration Denial, CPTHCPCService Being Disputed, Explanation of Your Request Please, Note If you are acting on the, You may mail your request to, AetnaProvider Resolution Team, and PO Box Lexington KY .
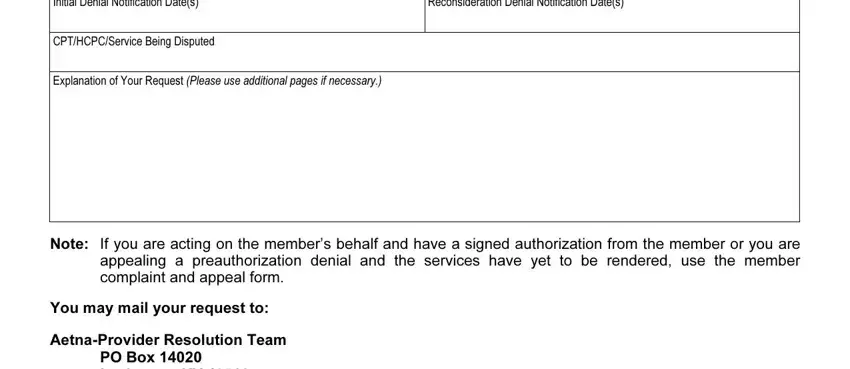
Those who work with this form generally make errors while filling out AetnaProvider Resolution Team in this area. Be certain to go over whatever you type in here.
Step 3: Soon after looking through your fields, press "Done" and you are good to go! After registering a7-day free trial account here, you will be able to download aetna practitioner and provider complaint and appeal form or email it promptly. The document will also be easily accessible through your personal account menu with your each and every edit. We don't share the information you type in when dealing with documents at our website.