The idea driving our PDF editor was to help it become as easy to use as possible. You'll find the overall procedure of managing aetna international medical claim form hassle-free should you follow the following steps.
Step 1: Click the "Get Form Here" button.
Step 2: At this point, you can start editing the aetna international medical claim form. The multifunctional toolbar is at your disposal - add, eliminate, adjust, highlight, and undertake other sorts of commands with the content material in the document.
Enter the data required by the system to prepare the form.
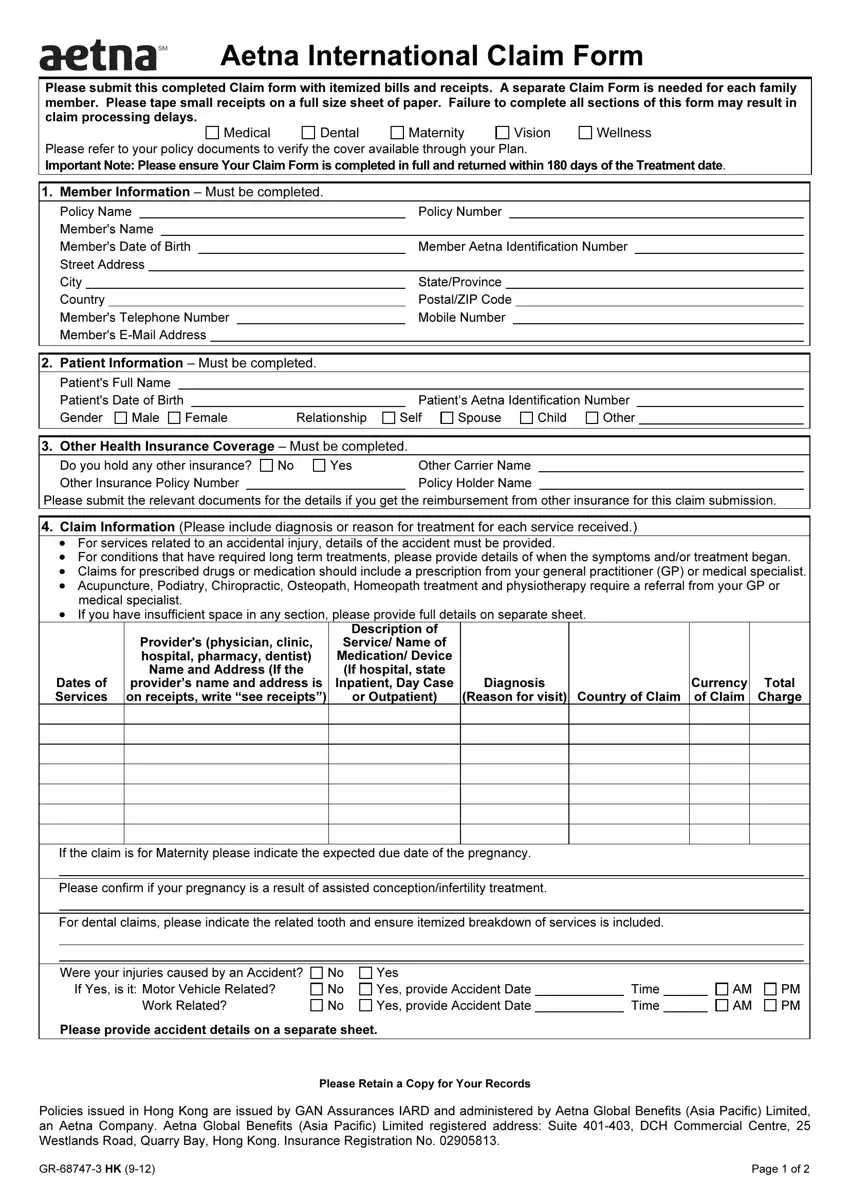
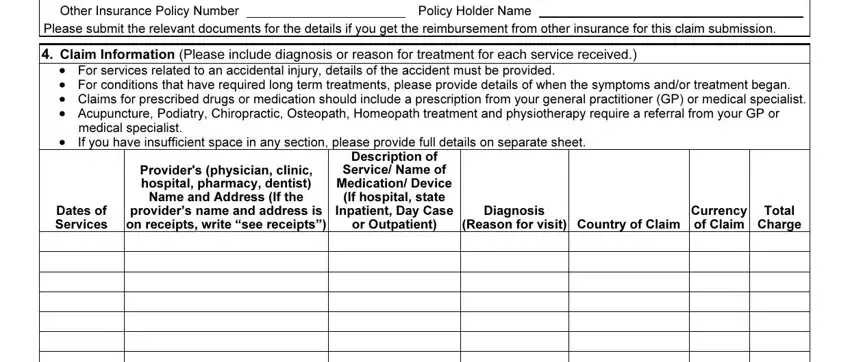
Make sure you provide your details in the box Other Health Insurance Coverage, Other Carrier Name Policy Holder, Yes, Claim Information Please include, cid For services related to an, medical specialist If you have, cid, Providers physician clinic, Dates of Services, Description of Service Name of, Diagnosis, Reason for visit Country of Claim, Currency of Claim, and Total Charge.
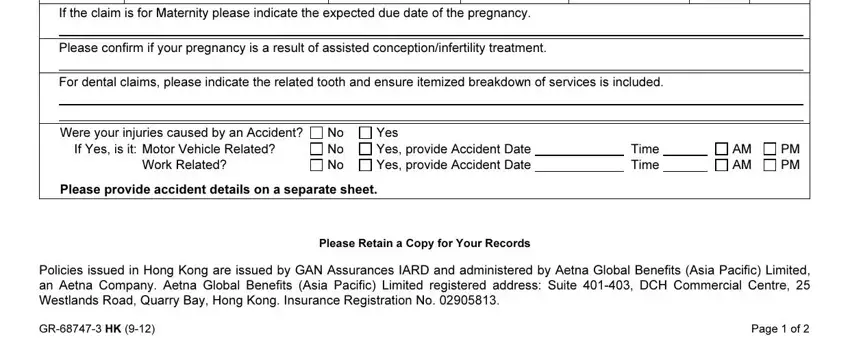
In the If the claim is for Maternity, Please confirm if your pregnancy, For dental claims please indicate, Were your injuries caused by an, Work Related, No No No, Yes Yes provide Accident Date Yes, Time Time, AM AM, PM PM, Please provide accident details on, Please Retain a Copy for Your, Policies issued in Hong Kong are, GR HK, and Page of area, point out the important information.
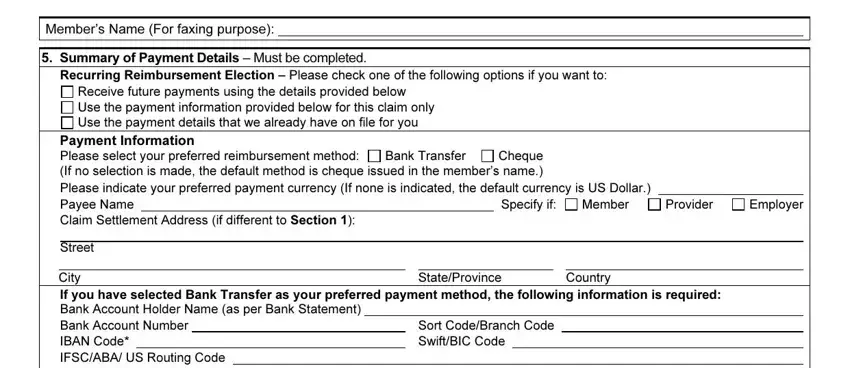
Within the section Members Name For faxing purpose, Summary of Payment Details Must, Receive future payments using the, Payment Information Please select, Cheque If no selection is made the, Bank Transfer, Please indicate your preferred, Specify if, Member, Provider, Employer, Street, City, StateProvince, and Country, identify the rights and obligations of the parties.
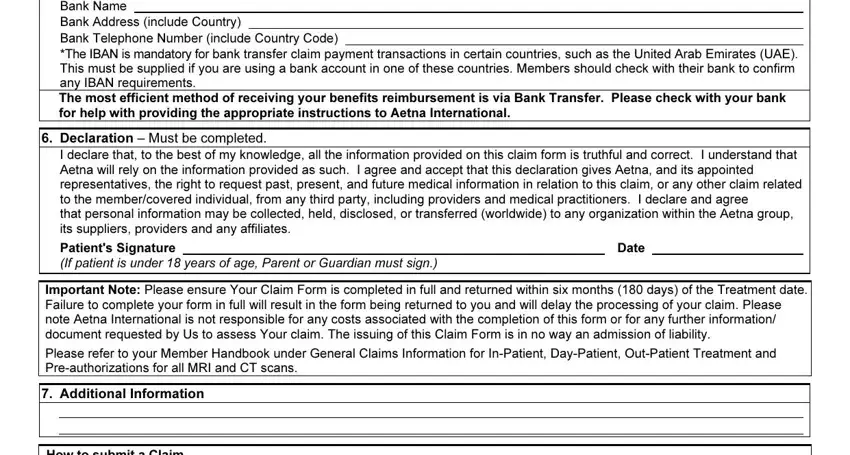
Check the sections Bank Name Bank Address include, The IBAN is mandatory for bank, Declaration Must be completed, I declare that to the best of my, Patients Signature, If patient is under years of age, Date, Important Note Please ensure Your, Additional Information, and How to submit a Claim Aetna and thereafter fill them in.
Step 3: Once you've hit the Done button, your form is going to be accessible for upload to each electronic device or email address you identify.
Step 4: Ensure that you keep away from potential complications by having a minimum of 2 copies of your document.
