N
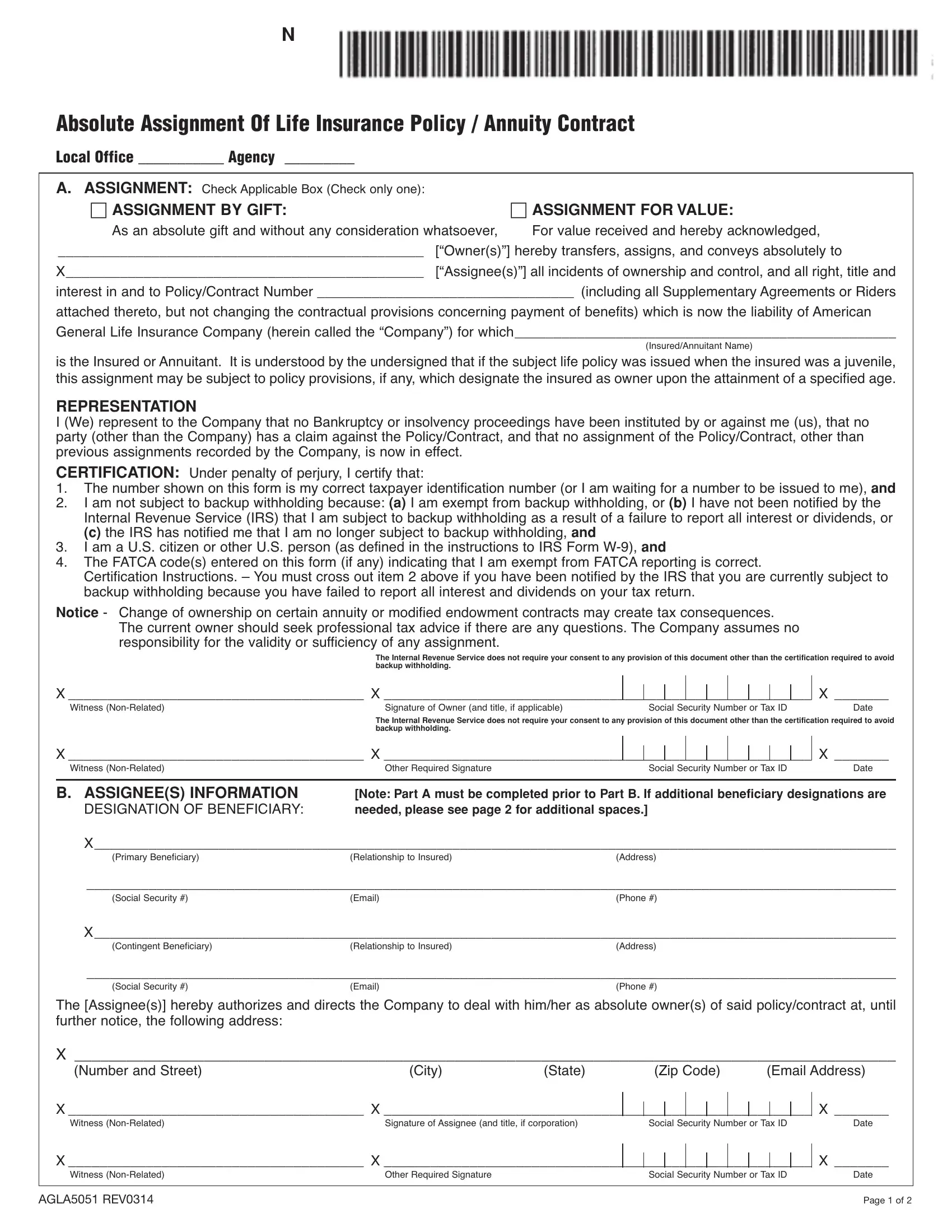
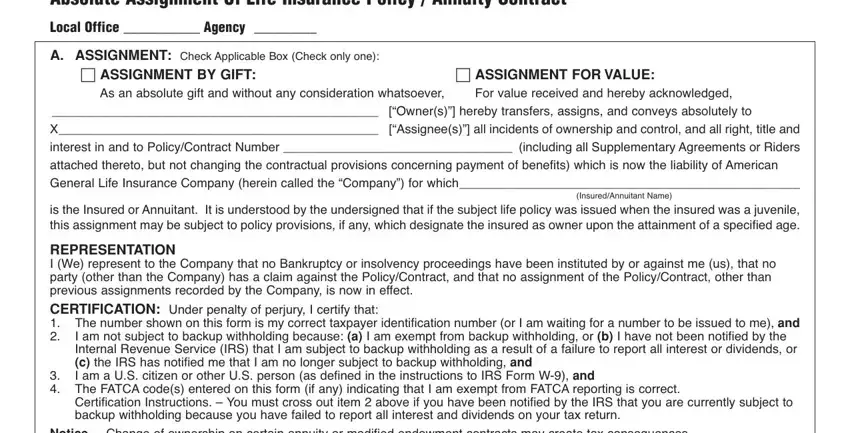
Absolute Assignment Of Life Insurance Policy / Annuity Contract
Local Office ___________ Agency _________
A.ASSIGNMENT: Check Applicable Box (Check only one):
c ASSIGNMENT BY GIFT: |
|
c ASSIGNMENT FOR VALUE: |
As an absolute gift and without any consideration whatsoever, |
For value received and hereby acknowledged, |
_______________________________________________ |
[“Owner(s)”] hereby transfers, assigns, and conveys absolutely to |
X______________________________________________ |
[“Assignee(s)”] all incidents of ownership and control, and all right, title and |
interest in and to Policy/Contract Number _________________________________ (including all SupplementaryAgreements or Riders
attached thereto, but not changing the contractual provisions concerning payment of benefits) which is now the liability of American General Life Insurance Company (herein called the “Company”) for which_________________________________________________
(Insured/Annuitant Name)
is the Insured orAnnuitant. It is understood by the undersigned that if the subject life policy was issued when the insured was a juvenile, this assignment may be subject to policy provisions, if any, which designate the insured as owner upon the attainment of a specified age.
REPRESENTATION
I (We) represent to the Company that no Bankruptcy or insolvency proceedings have been instituted by or against me (us), that no party (other than the Company) has a claim against the Policy/Contract, and that no assignment of the Policy/Contract, other than previous assignments recorded by the Company, is now in effect.
CERTIFICATION: Under penalty of perjury, I certify that:
1.The number shown on this form is my correct taxpayer identification number (or I am waiting for a number to be issued to me), and
2.I am not subject to backup withholding because: (a) I am exempt from backup withholding, or (b) I have not been notified by the Internal Revenue Service (IRS) that I am subject to backup withholding as a result of a failure to report all interest or dividends, or
(c) the IRS has notified me that I am no longer subject to backup withholding, and
3.I am a U.S. citizen or other U.S. person (as defined in the instructions to IRS Form W-9), and
4.The FATCA code(s) entered on this form (if any) indicating that I am exempt from FATCA reporting is correct.
Certification Instructions. – You must cross out item 2 above if you have been notified by the IRS that you are currently subject to backup withholding because you have failed to report all interest and dividends on your tax return.
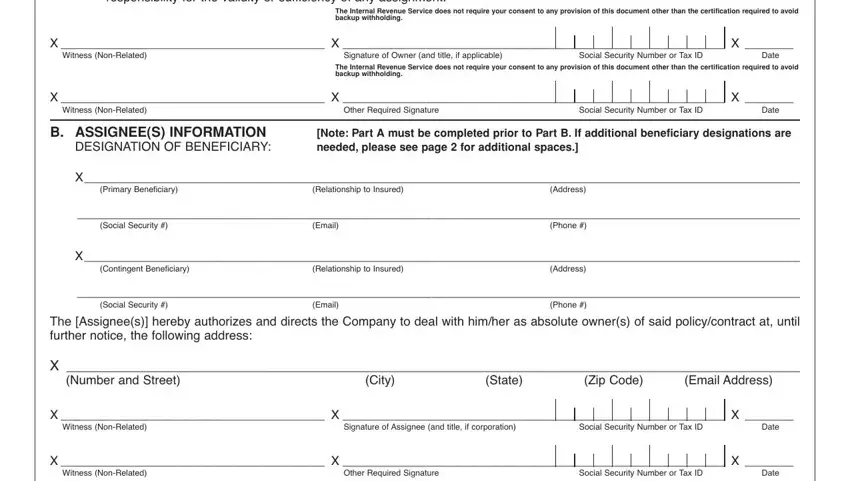
Notice - Change of ownership on certain annuity or modified endowment contracts may create tax consequences. The current owner should seek professional tax advice if there are any questions. The Company assumes no responsibility for the validity or sufficiency of any assignment.
The Internal Revenue Service does not require your consent to any provision of this document other than the certification required to avoid backup withholding.
X______________________________________ X _______________________________________________________ X _______
Witness (Non-Related)Signature of Owner (and title, if applicable) Social Security Number or Tax ID Date
The Internal Revenue Service does not require your consent to any provision of this document other than the certification required to avoid backup withholding.
X______________________________________ X _______________________________________________________ X _______
Witness (Non-Related)Other Required SignatureSocial Security Number or Tax ID Date
B. ASSIGNEE(S) INFORMATION |
[Note: Part A must be completed prior to Part B. If additional beneficiary designations are |
DESIGNATION OF BENEFICIARY: |
needed, please see page 2 for additional spaces.] |
X_______________________________________________________________________________________________________ |
(Primary Beneficiary) |
(Relationship to Insured) |
(Address) |
________________________________________________________________________________________________________
(Social Security #)(Email)(Phone #)
X_______________________________________________________________________________________________________
(Contingent Beneficiary)(Relationship to Insured)(Address)
________________________________________________________________________________________________________
(Social Security #) |
(Email) |
(Phone #) |
The [Assignee(s)] hereby authorizes and directs the Company to deal with him/her as absolute owner(s) of said policy/contract at, until further notice, the following address:
X _______________________________________________________________________________________________ |
(Number and Street) |
(City) |
(State) |
(Zip Code) |
(Email Address) |
X______________________________________ X _______________________________________________________ |
|
|
|
|
|
|
|
|
|
X _______ |
|
|
|
|
|
Witness (Non-Related) |
Signature of Assignee (and title, if corporation) |
Social Security Number or Tax ID |
Date |
|
|
|
|
|
|
X______________________________________ X _______________________________________________________ |
|
|
|
|
|
X _______ |
Witness (Non-Related) |
Other Required Signature |
|
Social Security Number or Tax ID |
Date |
|
|
|
|
|
|
|
|
|
|
AGLA5051 REV0314 |
|
|
|
|
|
|
|
|
Page 1 of 2 |
B.ASSIGNEE(S) INFORMATION
DESIGNATION OF PRIMARY BENEFICIARY:
X_______________________________________________________________________________________________________
(Name)(Relationship to Insured)(Address)
________________________________________________________________________________________________________
(Social Security #)(Email)(Phone #)
X_______________________________________________________________________________________________________
(Name)(Relationship to Insured)(Address)
________________________________________________________________________________________________________
(Social Security #)(Email)(Phone #)
DESIGNATION OF CONTINGENT BENEFICIARY:
X_______________________________________________________________________________________________________
(Name)(Relationship to Insured)(Address)
________________________________________________________________________________________________________
(Social Security #)(Email)(Phone #)
X_______________________________________________________________________________________________________
(Name)(Relationship to Insured)(Address)
________________________________________________________________________________________________________
(Social Security #) |
(Email) |
(Phone #) |
American General Life Insurance Company
P O Box 305355 • Nashville, TN 37230-5355
© 2014 American International Group, Inc. (AIG). All rights reserved.
AGLA5051 REV0314 |
Page 2 of 2 |