
Through the online PDF tool by FormsPal, you'll be able to fill in or alter ahca form 5220 001 here and now. Our development team is continuously endeavoring to enhance the tool and help it become even easier for users with its cutting-edge features. Enjoy an ever-improving experience now! With a few easy steps, you can begin your PDF editing:
Step 1: Press the orange "Get Form" button above. It'll open up our editor so you can start filling in your form.
Step 2: After you launch the tool, you will get the document ready to be completed. Apart from filling in different blanks, you might also do many other things with the PDF, namely putting on any text, editing the original text, adding graphics, putting your signature on the form, and a lot more.
Pay attention while filling in this form. Make certain every single blank is filled out correctly.
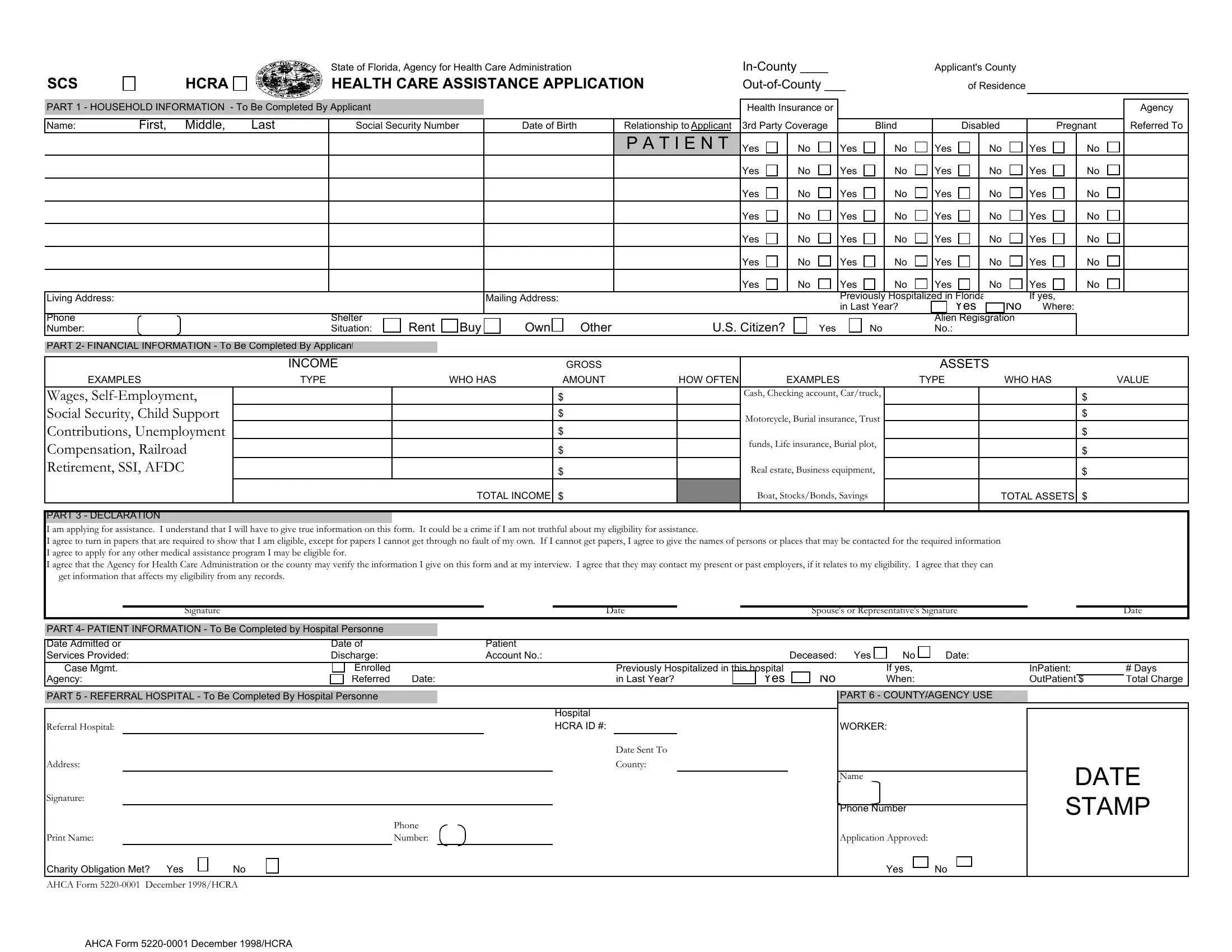
1. It is important to fill out the ahca form 5220 001 correctly, therefore pay close attention when working with the areas that contain all of these blanks:
2. Now that the last array of fields is done, you should add the needed details in TOTAL INCOME, Boat StocksBonds Savings, TOTAL ASSETS , PART DECLARATION I am applying, Signature, Date, Spouses or Representatives, Date, PART PATIENT INFORMATION To Be, Date of Discharge, Patient Account No, Case Mgmt, Agency, Enrolled Referred, and Date in order to move on to the 3rd step.
It is possible to make a mistake while filling in your Spouses or Representatives, consequently be sure you take a second look before you decide to send it in.
Step 3: Proofread what you've typed into the form fields and hit the "Done" button. Find your ahca form 5220 001 the instant you subscribe to a free trial. Readily access the pdf file in your FormsPal cabinet, with any modifications and adjustments conveniently preserved! FormsPal guarantees your data privacy via a secure system that in no way saves or distributes any type of personal information used in the PDF. Be confident knowing your documents are kept protected whenever you use our service!