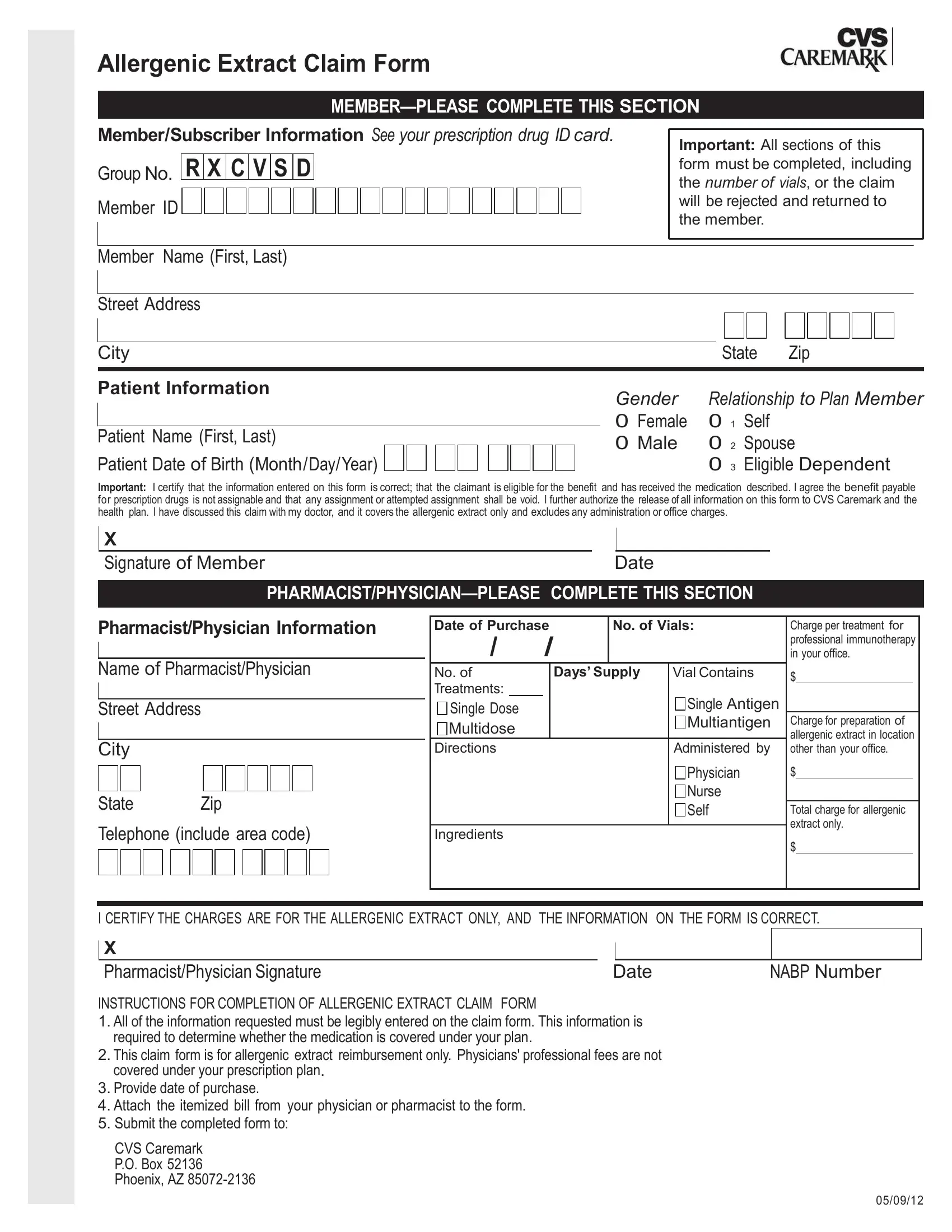
When navigating the healthcare landscape, especially for those dealing with allergies, understanding how to properly utilize the Allergenic Extract Claim Form is crucial. This form is designed for members who need to submit a claim for reimbursement for allergenic extracts. It's a key piece of documentation that ensures members are reimbursed for the expenses incurred from their treatment, but there's a catch; every section of the form must be filled out meticulously, including specifying the number of vials, or else the claim gets rejected. The form requires basic subscriber information, details about the patient, and an assertion from the member that all the information provided is correct and that the allergenic extract has been received. It goes a step further to mandate that only charges related to the allergenic extract are claimable, excluding any fees tied to the administration or office visits. On the flip side, pharmacists or physicians also have a section to complete, providing details about the treatment, including the number of vials and the cost, alongside certifying that the charges are exclusively for the allergenic extract. For a claim to be processed successfully, the completed form, together with an itemized bill from the healthcare provider, must be sent to a specified address. This underscores the importance of accurately completing the form to ensure that the reimbursement process is seamless and efficient, providing a crucial support system for individuals managing their allergy treatments.
| Question | Answer |
|---|---|
| Form Name | Allergenic Extract Claim Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Allergenic, RX, CVSD, cvs allergenic extraxt claim form |
Allergenic Extract Claim Form
Member/Subscriber Information See your prescription drug ID card. |
Important: All sections of this |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Group No. |
R |
X |
C |
V |
S |
D |
|
|
|
|
|
|
|
|
|
|
|
|
|
form must be completed, including |
|
|
the number of vials, or the claim |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Member ID |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
will be rejected and returned to |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
the member. |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Member Name (First, Last)
Street Address |
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
Zip |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Patient Information |
Gender |
Relationship to Plan Member |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
0 Female |
0 1 |
Self |
|
|
|
|
|
|
||||
Patient Name (First, Last) |
|
|
|
|
|
|
||||||||||||||||||
0 Male |
0 2 |
Spouse |
||||||||||||||||||||||
Patient Date of Birth (Month/Day/Year) |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
0 3 |
Eligible Dependent |
|||||||||||
Important: I certify that the information entered on this form is correct; that the claimant is eligible for the benefit and has received the medication described. I agree the benefit payable for prescription drugs is not assignable and that any assignment or attempted assignment shall be void. I further authorize the release of all information on this form to CVS Caremark and the health plan. I have discussed this claim with my doctor, and it covers the allergenic extract only and excludes any administration or office charges.
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
Signature of Member |
|
|
|
|
|
|
|
|
Date |
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
Pharmacist/Physician Information |
|
Date of Purchase |
|
|
|
No. of Vials: |
Charge per treatment for |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
/ |
|
/ |
|
|
|
|
|
|
professional immunotherapy |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
in your office. |
|||||
Name of Pharmacist/Physician |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
No. of |
|
Days’ Supply |
Vial Contains |
$ |
|
||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Treatments: |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Single Antigen |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Street Address |
|
Single Dose |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
Multiantigen |
Charge for preparation of |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Multidose |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
allergenic extract in location |
||||
City |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Directions |
|
|
|
|
|
|
Administered by |
other than your office. |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician |
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Nurse |
|
|
|
|
State |
Zip |
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
Self |
Total charge for allergenic |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Telephone (include area code) |
|
|
|
|
|
|
|
|
|
|
|
extract only. |
||||||||||||||||||||||
|
Ingredients |
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
$ |
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I CERTIFY THE CHARGES ARE FOR THE ALLERGENIC EXTRACT ONLY, AND THE INFORMATION ON THE FORM IS CORRECT. |
||||||||||||||||||||||||||||||||||
|
|
X |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
Pharmacist/Physician Signature |
|
|
|
|
|
|
|
Date |
|
NABP Number |
||||||||||||||||||||||
INSTRUCTIONS FOR COMPLETION OF ALLERGENIC EXTRACT CLAIM FORM
1.All of the information requested must be legibly entered on the claim form. This information is required to determine whether the medication is covered under your plan.
2.This claim form is for allergenic extract reimbursement only. Physicians' professional fees are not covered under your prescription plan.
3.Provide date of purchase.
4.Attach the itemized bill from your physician or pharmacist to the form.
5.Submit the completed form to:
CVS Caremark P.O. Box 52136 Phoenix, AZ
05/09/12