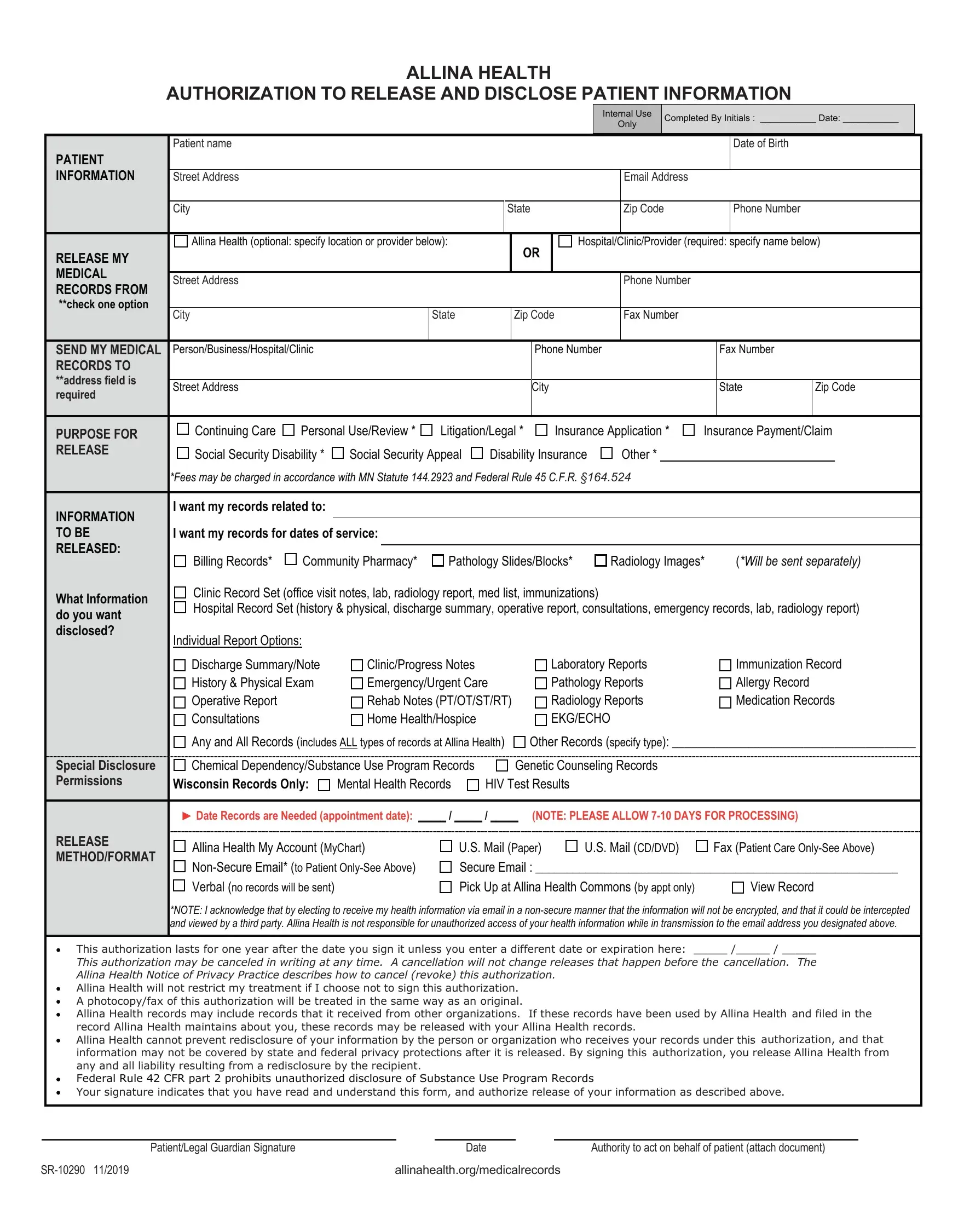
ALLINA HEALTH
AUTHORIZATION TO RELEASE AND DISCLOSE PATIENT INFORMATION
Completed By Initials : ___________ Date: ___________
|
|
Patient name |
|
|
|
|
|
|
|
|
|
|
|
|
|
Date of Birth |
|
|
|
PATIENT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
INFORMATION |
Street Address |
|
|
|
|
|
|
|
|
|
Email Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
|
State |
|
Zip Code |
|
|
Phone Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Allina Health (optional: specify location or provider below): |
|
|
OR |
|
Hospital/Clinic/Provider (required: specify name below) |
|
RELEASE MY |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
|
|
|
|
|
|
|
|
Phone Number |
|
|
|
|
|
|
RECORDS FROM |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
**check one option |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
State |
|
|
Zip Code |
|
Fax Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SEND MY MEDICAL |
Person/Business/Hospital/Clinic |
|
|
|
|
|
Phone Number |
|
|
|
Fax Number |
|
|
|
RECORDS TO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
**address field is |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address |
|
|
|
|
|
|
City |
|
|
|
|
State |
Zip Code |
|
required |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PURPOSE FOR |
Continuing Care |
Personal Use/Review * |
Litigation/Legal * |
Insurance Application * |
Insurance Payment/Claim |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RELEASE |
Social Security Disability * |
Social Security Appeal |
Disability Insurance |
Other * |
|
|
|
|
|
|
|
|
|
|
|
|
|
*Fees may be charged in accordance with MN Statute 144.2923 and Federal Rule 45 C.F.R. §164.524
I want my records related to:
|
|
|
INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TO BE |
I want my records for dates of service: |
|
|
|
|
|
|
|
|
|
|
|
RELEASED: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
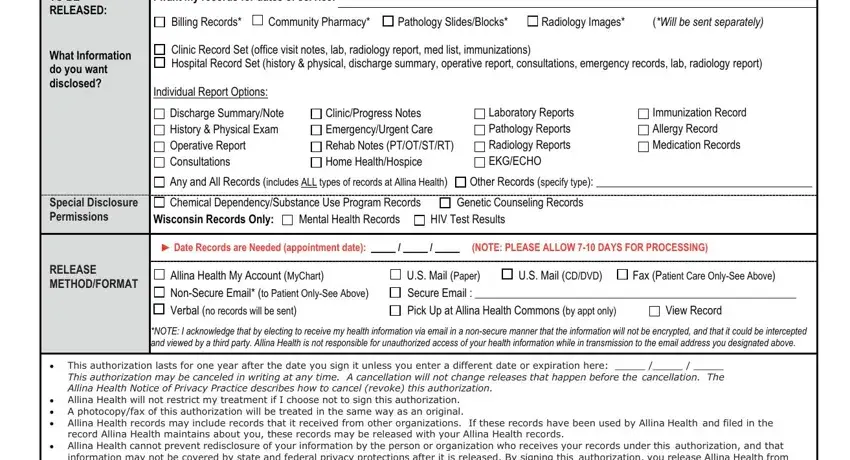
Billing Records* |
Community Pharmacy* |
Pathology Slides/Blocks* |
Radiology Images* |
(*Will be sent separately) |
|
|
|
|
|
|
|
What Information |
Clinic Record Set (office visit notes, lab, radiology report, med list, immunizations) |
|
|
|
|
|
Hospital Record Set (history & physical, discharge summary, operative report, consultations, emergency records, lab, radiology report) |
|
|
|
do you want |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
disclosed? |
Individual Report Options: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Discharge Summary/Note |
Clinic/Progress Notes |
|
|
Laboratory Reports |
Immunization Record |
|
|
|
|
History & Physical Exam |
Emergency/Urgent Care |
Pathology Reports |
Allergy Record |
|
|
|
|
Operative Report |
|
|
Rehab Notes (PT/OT/ST/RT) |
Radiology Reports |
Medication Records |
|
|
|
|
Consultations |
|
|
Home Health/Hospice |
|
|
EKG/ECHO |
|
|
|
|
|
|
Any and All Records (includes ALL types of records at Allina Health) |
Other Records (specify type): _______________________________________ |
|
|
|
|
Chemical Dependency/Substance Use Program Records |
Genetic Counseling Records |
|
|
|
|
|
Special Disclosure |
|
|
|
|
|
Permissions |
Wisconsin Records Only: |
Mental Health Records |
HIV Test Results |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date Records are Needed (appointment date): _____ / _____ / _____ |
(NOTE: PLEASE ALLOW 7-10 DAYS FOR PROCESSING) |
|
|
|
RELEASE |
Allina Health My Account (MyChart) |
U.S. Mail (Paper) |
U.S. Mail (CD/DVD) |
Fax (Patient Care Only-See Above) |
|
|
|
METHOD/FORMAT |
|
|
|
Non-Secure Email* (to Patient Only-See Above) |
Secure Email : __________________________________________________________ |
|
|
|
|
|
|
|
|
Verbal (no records will be sent) |
|
|
|
Pick Up at Allina Health Commons (by appt only) |
View Record |
|
|
|
|
*NOTE: I acknowledge that by electing to receive my health information via email in a non-secure manner that the information will not be encrypted, and that it could be intercepted |
|
|
|
|
and viewed by a third party. Allina Health is not responsible for unauthorized access of your health information while in transmission to the email address you designated above. |
|
|
|
|
|
|
|
|
|
|
|
|
This authorization lasts for one year after the date you sign it unless you enter a different date or expiration here: _____ /_____ / _____ |
|
|
|
This authorization may be canceled in writing at any time. A cancellation will not change releases that happen before the cancellation. The |
|
|
|
Allina Health Notice of Privacy Practice describes how to cancel (revoke) this authorization. |
|
|
|
|
|
|
Allina Health will not restrict my treatment if I choose not to sign this authorization. |
|
|
|
|
|
|
|
|
A photocopy/fax of this authorization will be treated in the same way as an original. |
|
|
|
|
|
|
|
|
Allina Health records may include records that it received from other organizations. If these records have been used by Allina Health and filed in the |
|
|
|
record Allina Health maintains about you, these records may be released with your Allina Health records. |
|
|
|
|
|
Allina Health cannot prevent redisclosure of your information by the person or organization who receives your records under this authorization, and that |
|
|
|
information may not be covered by state and federal privacy protections after it is released. By signing this authorization, you release Allina Health from |
|
|
|
any and all liability resulting from a redisclosure by the recipient. |
|
|
|
|
|
|
|
|
|
|
|
Federal Rule 42 CFR part 2 prohibits unauthorized disclosure of Substance Use Program Records |
|
|
|
|
|
Your signature indicates that you have read and understand this form, and authorize release of your information as described above. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient/Legal Guardian Signature |
|
|
|
|
|
Date |
|
|
Authority to act on behalf of patient (attach document) |
|
SR-10290 11/2019 |
|
|
|
|
allinahealth.org/medicalrecords |
|
|
|
Directions for Completion of Form
Patient Information: Complete the entire section which identifies clearly and legibly all of the demographic information specific to the patient (individual about whom information is being requested)
Release My Medical Records From: Check the first box if you would like your records released from an Allina Health facility/provider. Check the second box if you are requesting your records be released from a non-Allina Health facility/provider. When checking the Allina Health option, please specify the specific Allina Health location you are seeking information from. Please be specific in your request. For example, United Hospital, St. Paul, MN; Buffalo Hospital, Buffalo, MN; Allina Medical Clinic Shoreview, Shoreview, MN. If you do not identify a specific hospital or clinic (e.g. Allina Health), records may be provided from ALL Allina Health hospitals or clinics where you have received care. Please see allinahealth.org/medical records for a listing of Allina Health hospital and clinic locations and addresses.
Send My Medical Records To: Identify the full name/business, address, phone and contact information with the name of the individual who is to receive the information. Please allow 7-10 days for all requests to be processed and sent to the recipient.
Purpose For Release: Please identify why you need a copy of your record. This helps us to track and assign a priority status to your request. It also informs us who may be responsible for the cost of records (where appropriate).
Information to Be Released: This section gives us the instructions for what information you want released. If you select “Clinic Record Set” or “Hospital Record Set”, we will disclose the pertinent documents that are specific to that type of patient care visit. This is typically what doctors’ offices, hospitals or other health care providers need to provide information related to your care. If you select “any and all” records, your entire record will be provided for a specific visit date or all dates. It is very helpful if you identify the date or range of dates, needed by the requestor. Please note record types listed in the Special Disclosure Permissions section must be checked in order for them to be released.
Release Method: This tells us how you would like your information delivered. If you wish to view information prior to selection of documents, please identify this on the authorization form and we will contact you to set up a viewing appointment. Please note that viewing appointments are done at the Allina Health Corporate Office in Minneapolis. If you wish information about you to be shared verbally or for an authorization to be on file for others to have access to your medical information, please write this in this section (example: form on file for access by my husband upon his specific request). Please note: there are size limitations when emailing records.
Duration of the authorization, revocation and other information you need to know: This authorization will automatically expire in 12 months unless you include a different date. You may indicate the authorization is valid “5 years”, “10 years”, but there needs to be an ending date (do not use terms such as “lifetime” or “forever”). The authorization can be revoked by your written direction to our organization.
Contact Information for Patient Record Copies
***Incoming medical records are not to be sent to this department***
Allina Health
Attn: Health Information/ROI – Mail Route 10203
PO Box 43
Minneapolis, MN 55440-0043
Phone: 612-262-2300
Fax: 612-262-2323
Email: MedicalRecords@allina.com
Contact Information for Allina Health Pharmacy Charges Copies Allina Health Pharmacy – Mail Route 10807
|
Allina Health |
-------------------------------------------- |
|
PO Box 43 |
|
|
|
Plate: Black |
|
Minneapolis, MN 55440-0043 |
|
|
|
Phone: |
612-262-5980 |
|
|
Fax: |
612-262-5988 |
|
|
For a list of Allina Health locations and addresses, please visit allinahealth.org |
|
|
SR-10290 11/2019 |
allinahealth.org/medicalrecords |
|
|
|
|
|