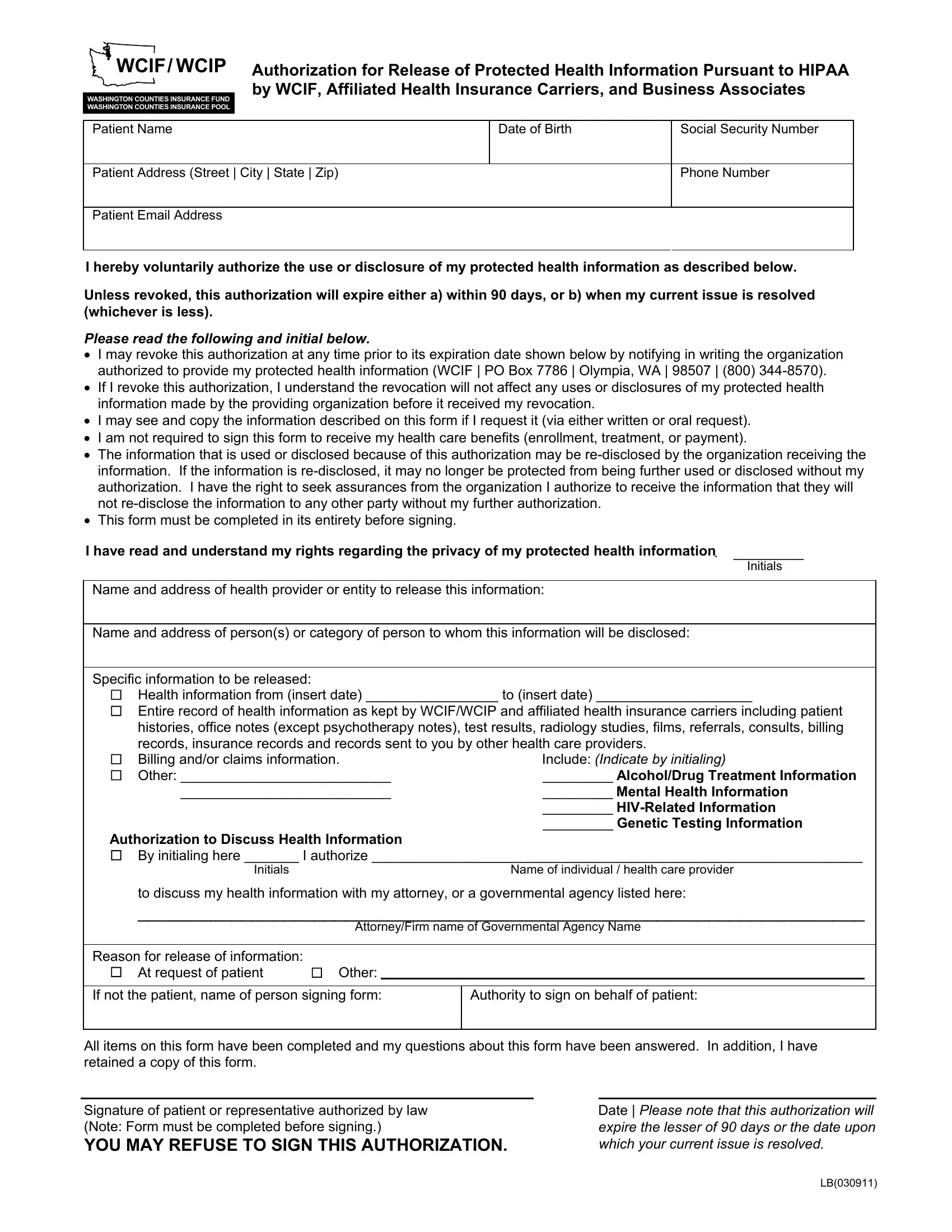
In today's healthcare landscape, the protection and lawful sharing of individual health information is paramount, guided by comprehensive federal regulations such as the Health Insurance Portability and Accountability Act (HIPAA). A core component ensuring compliance and respect for patient privacy is the WCIF/WCIP Authorization for Release of Protected Health Information form. This document serves a critical function within Washington Counties Insurance Fund (WCIF) and Washington Counties Insurance Pool (WCIP), facilitating the authorized exchange of protected health records between healthcare providers, insurance carriers, and other relevant entities. It outlines the conditions under which a patient's health information can be disclosed, emphasizing the voluntary nature of such disclosures. Specifically, it addresses the fundamentals around patient consent, the scope of information to be shared, the duration of the authorization, and the rights of the patient regarding the revocation of consent and access to their information. It also underscores that executing this form is not a prerequisite for receiving health care benefits, while illuminated is the potential for re-disclosure by third parties, which may no longer protect the information under HIPAA. The content and completion requirements of the form are designed to ensure patients are fully informed and consenting participants in the management of their health information. This highlights a balance between regulatory compliance and the empowerment of patients in the decision-making processes related to their personal health data.
| Question | Answer |
|---|---|
| Form Name | Wcif Form Lb |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Authorization for Release of PHI kansas 2015 hipaa consebnt form for patient printable |
