
Using FormsPal's free PDF editor, you can complete the Allina Hospitals and Clinics authorization form entirely online without downloading special software. Follow the steps below to fill out, sign, and save your completed Allina health release of information form.
Step 1: Click the "Get Form" button at the top of this page to open the Allina authorization form in FormsPal's secure online editor.
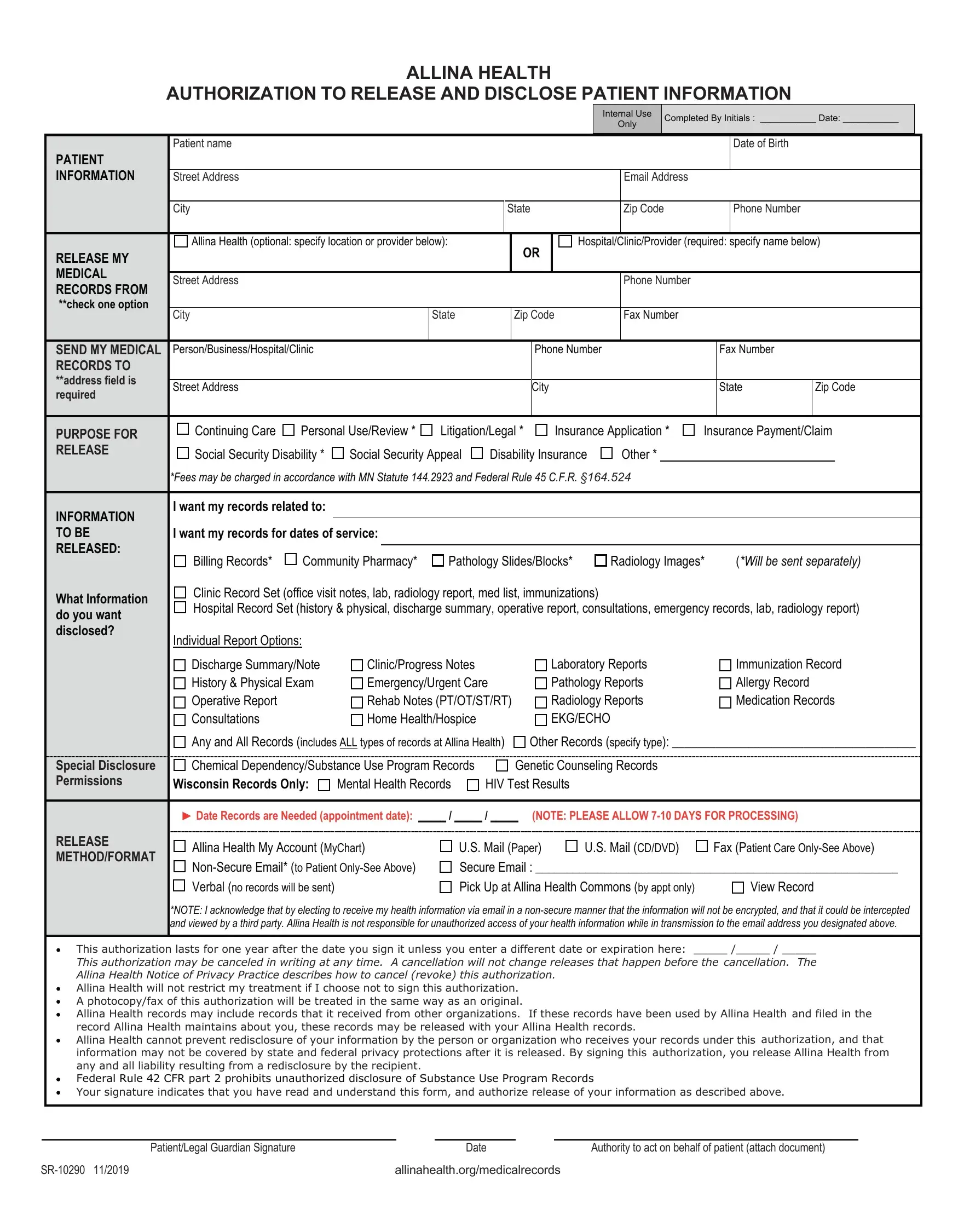
Step 2: Begin entering your patient information in the first section of the form. Fill in your personal and contact details accurately:
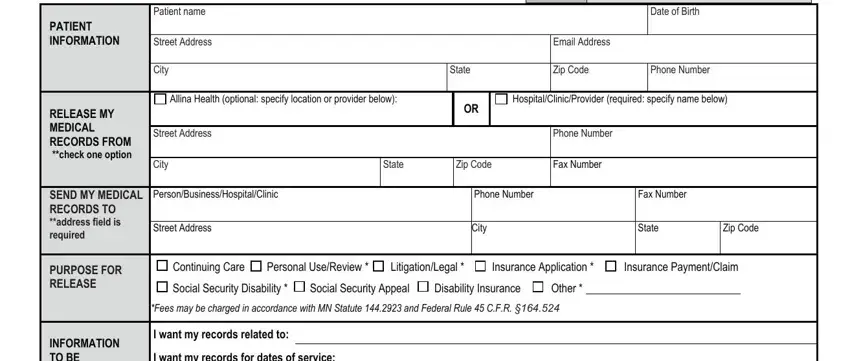
Step 3: Complete the authorization details. Specify whether you want records transferred from or to Allina Health, select the purpose of release, and indicate the type of records needed. Fields include INFORMATION TO BE RELEASED, What Information do you want, I want my records for dates of, Billing Records, Community Pharmacy Pathology, Clinic Record Set office visit, Individual Report Options, Discharge Summary/Note History, Clinic/Progress Notes, Laboratory Reports/Pathology, Immunization Record/Allergy Record, Any and All Records, Special Disclosure Permissions, Chemical Dependency/Substance Use, and Mental Health Records/HIV Test:
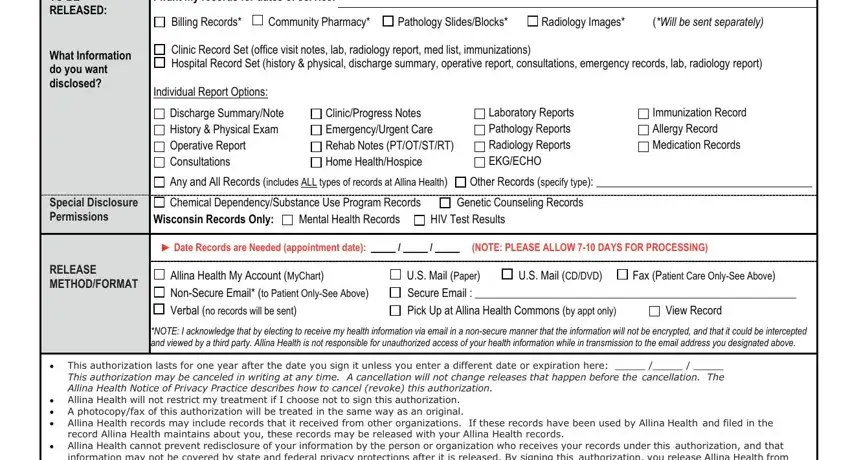
Step 4: In the final section, review and complete the authorization duration and signature fields: This authorization lasts for one (year), Patient/Legal Guardian Signature, Date, and Authority to act on behalf of. Take care with the Authority to act field and review it before finalizing:

Step 5: Review all entries for accuracy. When complete, click "Done" to save or download your completed Allina authorization form as a PDF. FormsPal does not share or sell any personal information you enter.
Frequently Asked Questions About the Allina Authorization Form
How long is the Allina authorization form valid?
The Allina health release of information authorization is valid for one year from the date of signing unless you specify a shorter period or revoke it beforehand. You may revoke the authorization at any time by contacting Allina Health medical records.
What records can I request using this form?
You can request any health records in Allina Health's possession, including clinic and hospital visits, billing records, radiology images, laboratory results, immunization records, discharge summaries, and specialized records such as mental health or substance use records. Minnesota law requires separate authorization for certain sensitive record categories.
Who can sign the Allina health authorization form?
The patient must sign if they are 18 or older. For minors, a parent or legal guardian may sign. If the patient is deceased or incapacitated, a personal representative, legal guardian, or power of attorney holder may authorize release on the patient's behalf.
Are there similar forms for other healthcare providers?
Yes. FormsPal also provides the United Healthcare release of information form, the Kaiser Permanente health information form, and the Hoag medical records request for other healthcare providers.