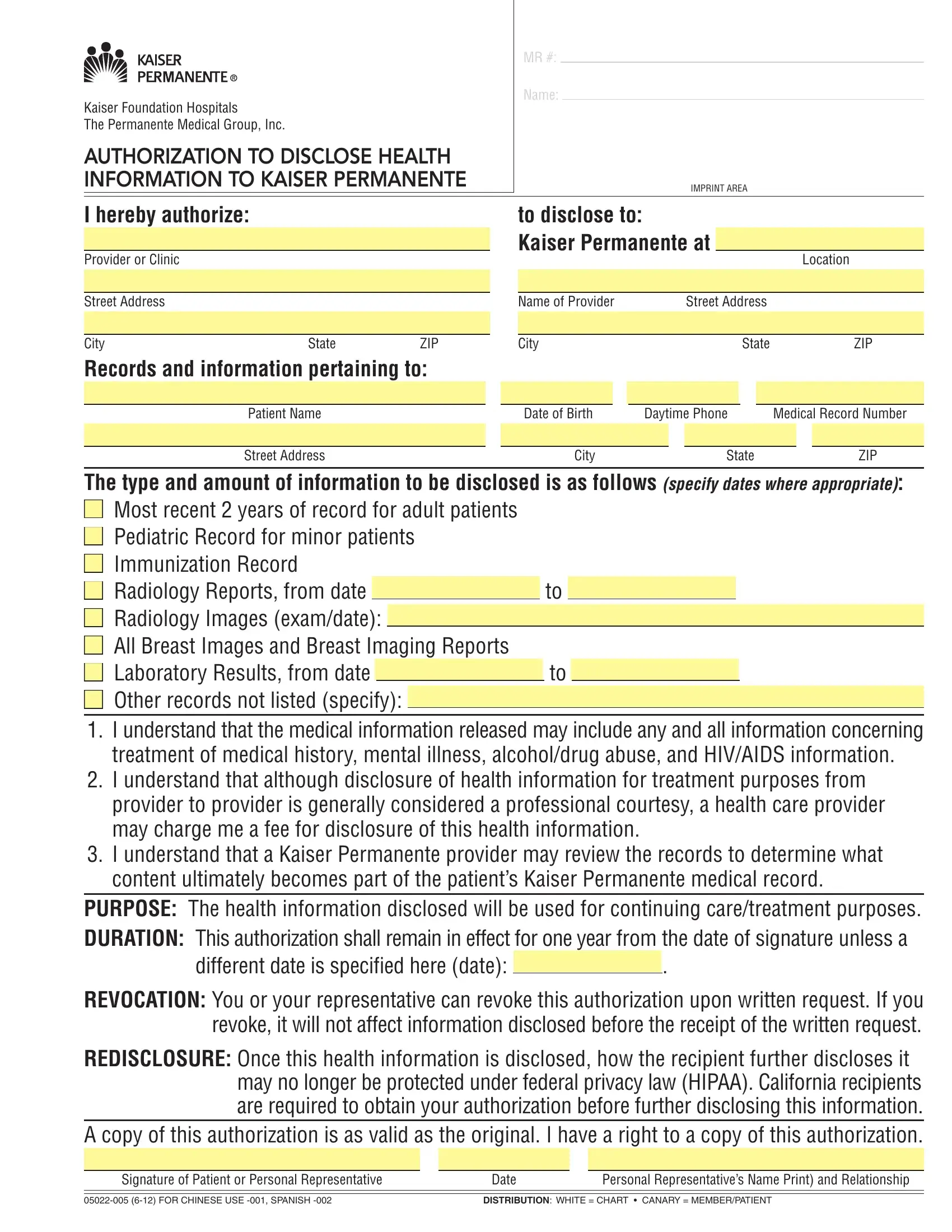
Navigating the complexities of sharing health information can be challenging, but the Health Information Kaiser Permanente form provides a structured and secure method for individuals to authorize the disclosure of their medical records. This form is an essential tool for patients of Kaiser Foundation Hospitals and The Permanente Medical Group, Inc., facilitating the seamless transfer of vital health information to Kaiser Permanente. It specifies the type and scope of records to be shared, ranging from the most recent two years of adult patient records to pediatric and immunization records, and even detailed reports like radiology and laboratory results. Importantly, the form addresses the inclusion of sensitive information, such as details of mental illness, alcohol or drug abuse, and HIV/AIDS, highlighting the comprehensive nature of the data transfer. Patients are made aware that while transferring records between providers is generally a courtesy, fees may apply, and they have the control to revoke the authorization at any time. The purpose behind this exchange is chiefly for the continuation of care or treatment, ensuring that healthcare providers have a full picture of the patient's medical history. Furthermore, this document outlines the protocol for how the information, once shared, will be incorporated into the patient’s Kaiser Permanente medical record, with a clear mention of how privacy is managed according to federal laws and California-specific regulations. The form underscores the patient's rights, including the ability to obtain a copy of the authorization, establishing a framework of trust and clarity in the sharing of health information.
| Question | Answer |
|---|---|
| Form Name | Health Information Kaiser Permanente Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | disclose information kaiser, medical kaiser disclosed, authorization disclose health information kaiser, health permanente information kaiser |