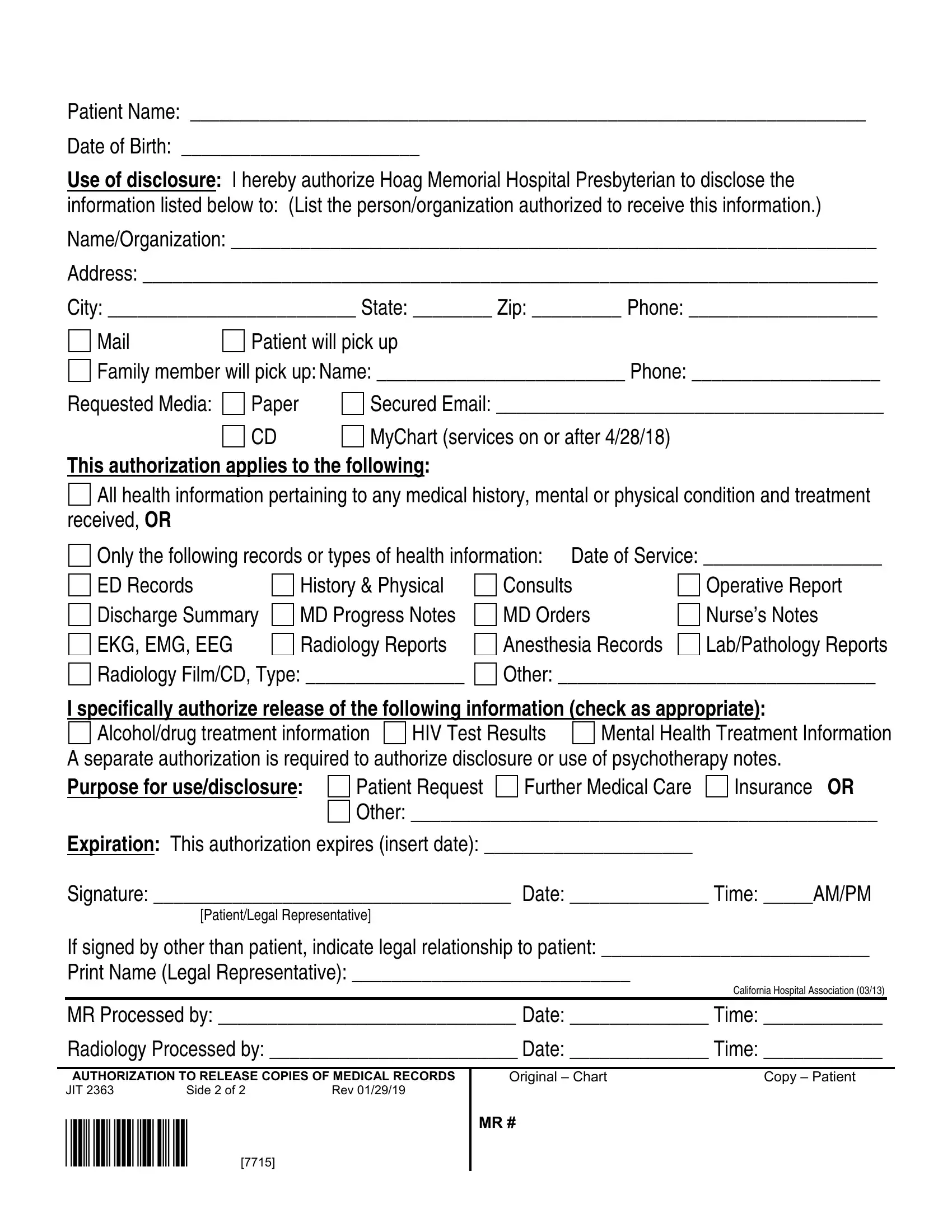
In today's healthcare landscape, the Hoag Medical Records form stands as a crucial document designed to facilitate the safe and regulated sharing of patient information among medical professionals, patients, and authorized third parties. This form, meticulously crafted by Hoag Memorial Hospital Presbyterian, serves multiple purposes, including but not limited to, enabling patients to request their medical records in various formats (such as paper, CD, or via secured email) and specifying the type of health information to be disclosed. Whether for continued medical care, insurance purposes, or personal records, patients have the flexibility to limit the disclosure to comprehensive health information or specific types of records such as lab reports, radiology reports, or mental health treatment details. Importantly, the form not only outlines the process for obtaining these records but also enshrines patient rights regarding the authorization of such disclosures. Essentially, by completing this document, patients authorize Hoag Memorial Hospital Presbyterian to release their medical information in accordance with California and Federal privacy laws, while also retaining the ability to revoke this authorization at any time. The thoughtful inclusion of protections against unauthorized re-disclosure underscores the form's role in safeguarding patient privacy, thereby embodying the delicate balance between the need for information sharing in healthcare and the imperative of protecting individual privacy.
| Question | Answer |
|---|---|
| Form Name | Hoag Medical Records Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 56 |
| Avg. time to fill out | 11 min 46 sec |
| Other names | hoag medical records fax, hoag release medical records, mychart hoag, hoag records |