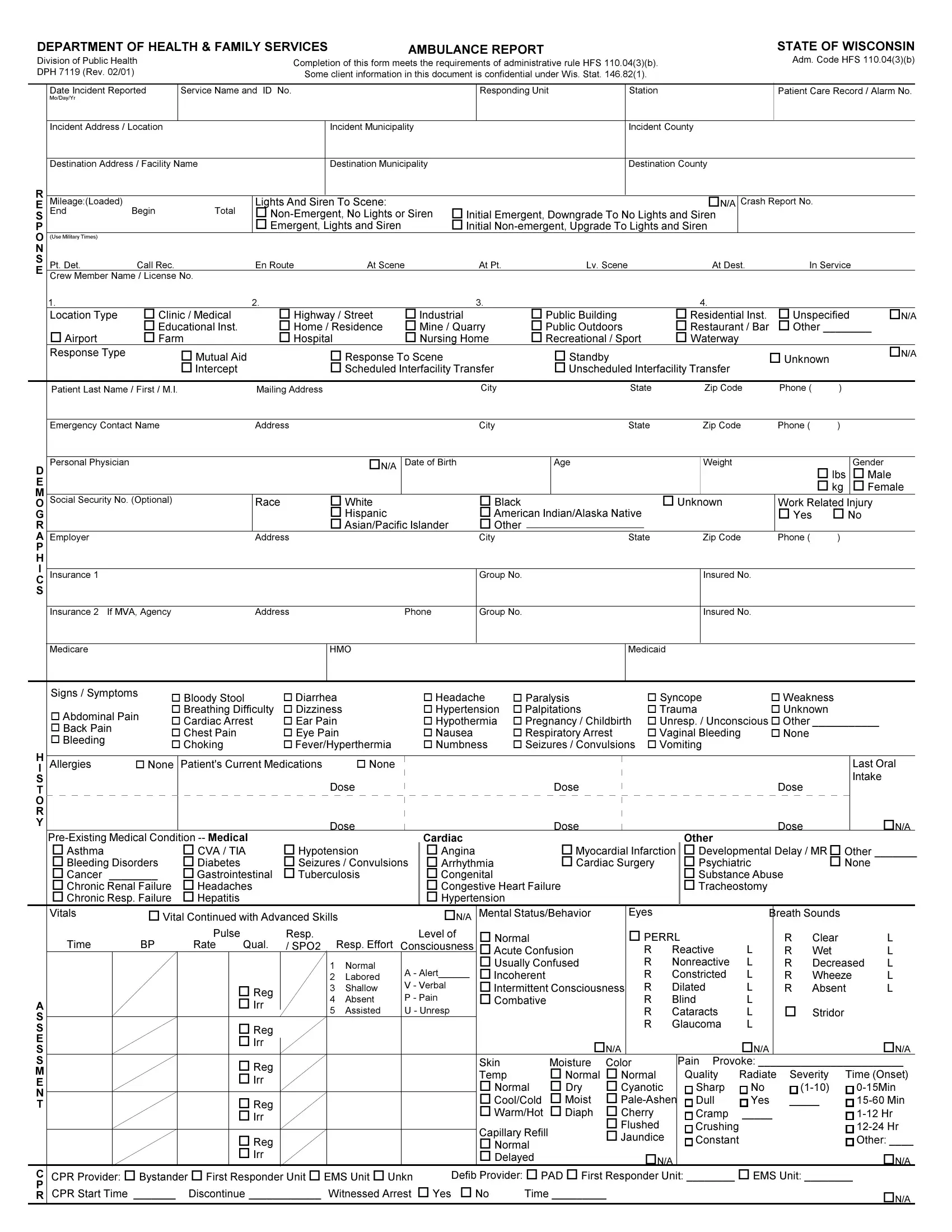
In the fast-paced environment of emergency health services, the Ambulance Report Form serves as a crucial document, meticulously designed to capture a wide array of information following an ambulance call. Issued by the Department of Health & Family Services, especially within the context of the State of Wisconsin, this form adheres strictly to the administrative rule HFS 110.04(3)(b), ensuring that all required data is systematically recorded. It begins with the basics such as the date of the incident, the service name and ID number, and detailed patient care record numbers, extending to more intricate details involving the incident's location, the patient's demographic information, and the medical response undertaken. Additionally, the form includes sections dedicated to capturing the patient's medical history, vital signs, the nature/cause of the injury or health issue, and any treatments provided by the emergency medical technicians (EMTs). The specificity of the form extends to recording the use of lights and siren during the transport, type of incident disposition, and even the status upon arrival at the destination. Furthermore, it acknowledges the importance of documenting interactions with other services on the scene and any difficulties encountered during the course of the emergency response. By transcoding such comprehensive information, the form not only aids in the immediate treatment and transport of patients but also contributes to the broader scope of healthcare analysis and policy formulation, ensuring that each response is well-documented for future reference, analysis, and potential improvement of emergency medical services.
| Question | Answer |
|---|---|
| Form Name | Ambulance Report Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | ambulance prf, patient report form ambulance pdf, patient report form app, patient report form ambulance |