
Handling PDF documents online is definitely a piece of cake using our PDF tool. You can fill out aoc 740 here painlessly. To retain our editor on the cutting edge of practicality, we strive to put into operation user-driven capabilities and improvements regularly. We are always looking for suggestions - assist us with revolutionizing PDF editing. Getting underway is simple! What you need to do is follow the next easy steps below:
Step 1: Access the PDF file in our editor by clicking the "Get Form Button" at the top of this webpage.
Step 2: The editor grants the capability to customize your PDF document in various ways. Enhance it with any text, correct original content, and include a signature - all when it's needed!
Filling out this form calls for focus on details. Make sure that each field is filled out accurately.
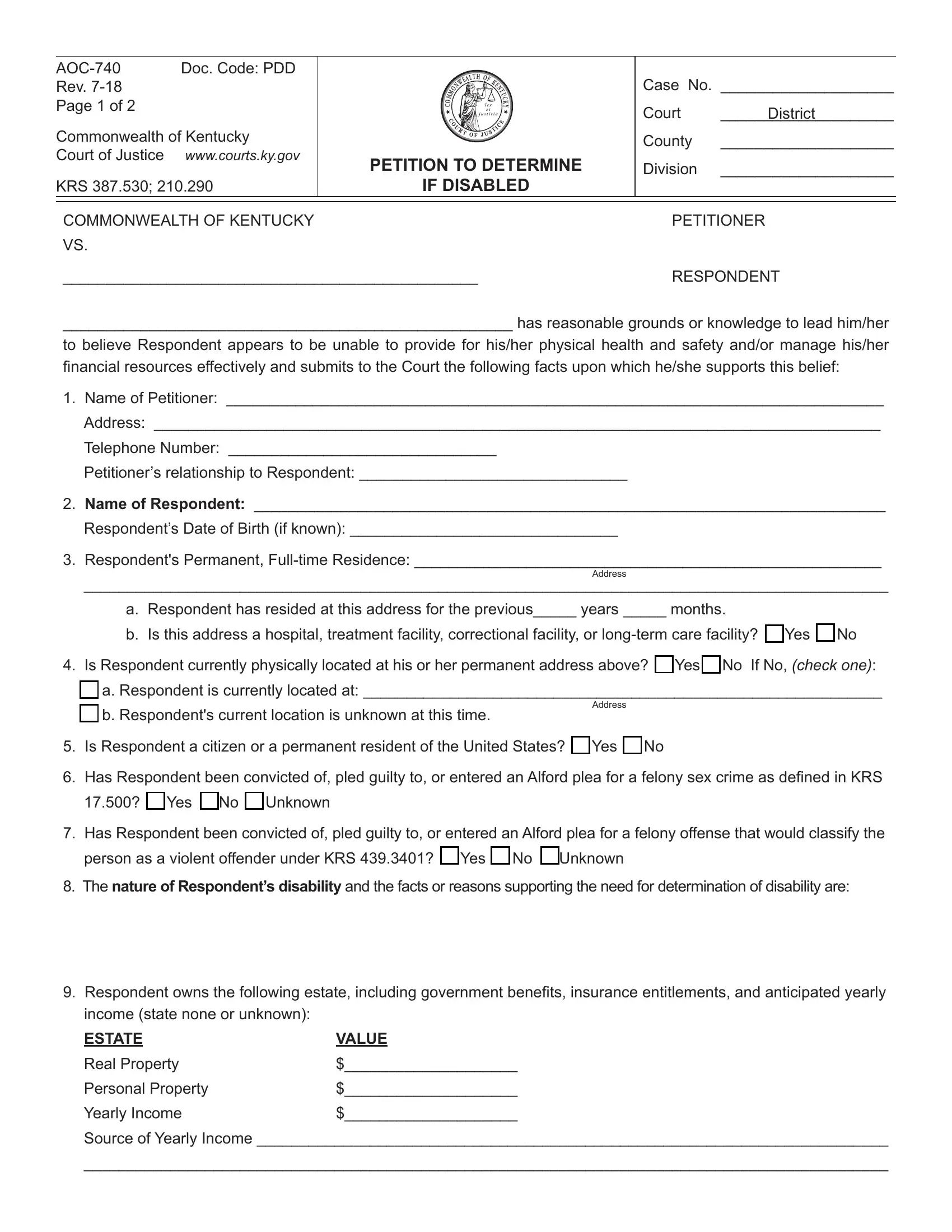
1. The aoc 740 needs specific information to be typed in. Be sure that the next blank fields are complete:
2. The next part would be to complete all of the following blanks: Name of Respondent , Respondents Date of Birth if known , Respondents Permanent Fulltime, Address, a Respondent has resided at this, Is Respondent currently, Address, Is Respondent a citizen or a, Has Respondent been convicted of, q Yes q No q Unknown, Has Respondent been convicted of, person as a violent offender under, The nature of Respondents, and Respondent owns the following.
3. This next step is generally simple - fill in all of the form fields in income state none or unknown ESTATE, VALUE, Real Property, Personal Property, Yearly Income, and Source of Yearly Income to complete this part.
4. All set to complete this fourth segment! Here you will have all of these AOC Rev Page of , Name of q Person or q Facility, Respondents next of kin Name , WHEREFORE Petitioner requests the, Trial by jury, and Counsel to represent the blank fields to fill out.
5. To wrap up your document, this particular segment has a few extra blank fields. Typing in Court appointment of a physician, Date, Signature of Petitioner, SUBSCRIBED and SWORN to before me, My Commission expires, County Kentucky, NameTitle, To be completed if Petitioner is, Attorneys Name , Address , Telephone Number , and Attorney Signature is going to finalize the process and you'll be done very quickly!
In terms of Court appointment of a physician and County Kentucky, be sure you double-check them in this current part. Those two are definitely the most significant fields in this document.
Step 3: Confirm that the details are correct and then press "Done" to proceed further. Right after starting a7-day free trial account here, you will be able to download aoc 740 or send it through email at once. The form will also be readily available via your personal cabinet with your modifications. Whenever you work with FormsPal, you'll be able to fill out documents without being concerned about database breaches or entries being distributed. Our secure software ensures that your personal information is maintained safely.