




When using the online tool for PDF editing by FormsPal, you'll be able to fill out or alter http benefitscal org here. To make our tool better and more convenient to use, we consistently come up with new features, with our users' feedback in mind. Starting is effortless! Everything you need to do is stick to the following simple steps down below:
Step 1: Press the "Get Form" button at the top of this webpage to open our tool.
Step 2: This tool will allow you to customize your PDF in a range of ways. Change it with your own text, correct original content, and place in a signature - all within a few mouse clicks!
Filling out this PDF requires attention to detail. Ensure all required fields are done accurately.
1. To get started, once filling in the http benefitscal org, start out with the form section that includes the subsequent blanks:

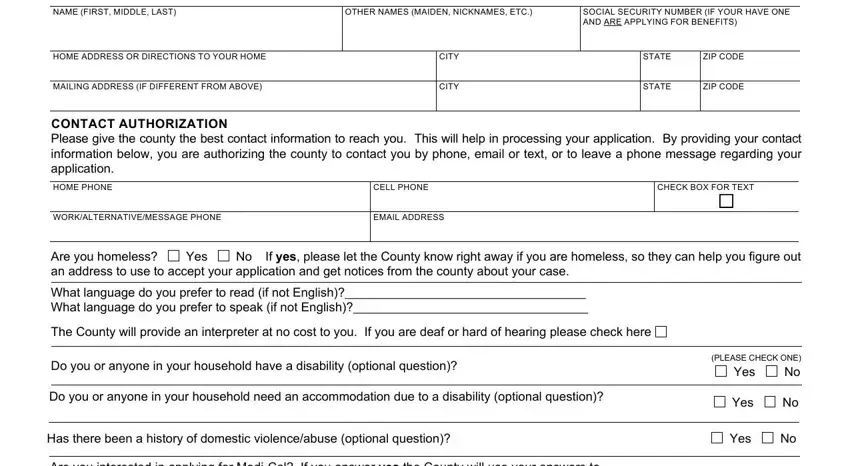
2. Just after this part is completed, proceed to type in the applicable details in all these - APPLICANTS INFORMATION, NAME FIRST MIDDLE LAST, OTHER NAMES MAIDEN NICKNAMES ETC, SOCIAL SECURITY NUMBER IF YOUR, HOME ADDRESS OR DIRECTIONS TO YOUR, MAILING ADDRESS IF DIFFERENT FROM, CITY, CITY, STATE, ZIP CODE, STATE, ZIP CODE, CONTACT AUTHORIZATION Please give, HOME PHONE, and CELL PHONE.
3. The following step is all about Are you interested in applying for, Is your households monthly gross, Is your households combined, Is your household a, Yes, Yes, Yes, Yes, I understand that by signing this, I read or had read to me the, My answers to the questions are, Any answers I may give for my, I read or had read to me and I, I read or had read to me the, and I understand that giving false or - type in every one of these fields.
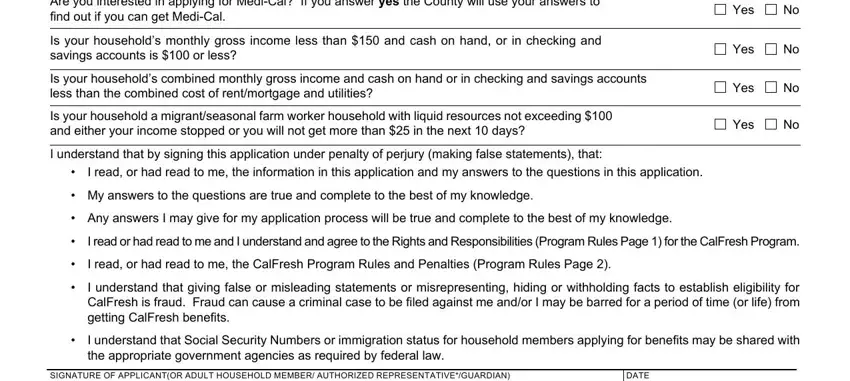
4. This subsection comes next with the following blank fields to complete: SIGNATURE OF APPLICANTOR ADULT, DATE, If you have an Authorized, CF REQUIRED FORM SUBSTITUTES, and PAGE OF .

5. Finally, this final segment is what you'll want to wrap up before finalizing the document. The fields here include the next: HOUSEHOLDS AUTHORIZED, Do you want to name someone to, Yes, If yes complete the following, AUTHORIZED REPRESENTATIVE PHONE, Do you want to name someone to, PHONE NUMBER, Yes, STREET ADDRESS, CITY, STATE, ZIP CODE, RACEETHNICITY Race and ethnicity, Check this box if you do not want, and this information for civil rights.
Always be very mindful while filling out this information for civil rights and RACEETHNICITY Race and ethnicity, since this is where a lot of people make mistakes.
Step 3: When you have reviewed the information in the document, click "Done" to finalize your form. Sign up with us now and easily use http benefitscal org, all set for download. Each and every edit you make is handily saved , so that you can edit the file later if necessary. FormsPal guarantees risk-free document editor with no personal information recording or sharing. Rest assured that your information is in good hands here!