Understanding how to navigate the use of an Application for Change of Beneficiary form is crucial for maintaining the accuracy and integrity of one's financial and estate planning. Companion of New York offers this form to policyholders who wish to make changes to their beneficiary designations, requiring careful attention to several guidelines and options provided. With an address at 3316 Farnam Street, Omaha, NE 68175, the company lays out specific instructions for policyholders on how to accurately complete and submit the form. Highlighted within are options for types of beneficiary designations including individual persons, trusts, corporations, partnerships, and even arrangements for unnamed children tied to a specific marriage. The form emphasizes the importance of using full names, avoiding adjustments after completion like corrections or erasures, and the necessity for witnessed signatures, especially when altering irrevocable beneficiaries or dealing with entities like corporations or partnerships. Additionally, the instructions delineate the paperwork required when submitting changes involving legal entities. This process, while it may seem daunting, is designed to safeguard the policyholder's intentions and ensure that the policy proceeds are allocated precisely as wished upon the policy’s maturity or in the event of the insured's death.
| Question | Answer |
|---|---|
| Form Name | Application Change Beneficiary Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | mutual of omaha change of beneficiary form, application change beneficiary, mutual of omaha life insurance change of beneficiary form, mutual omaha beneficiary |
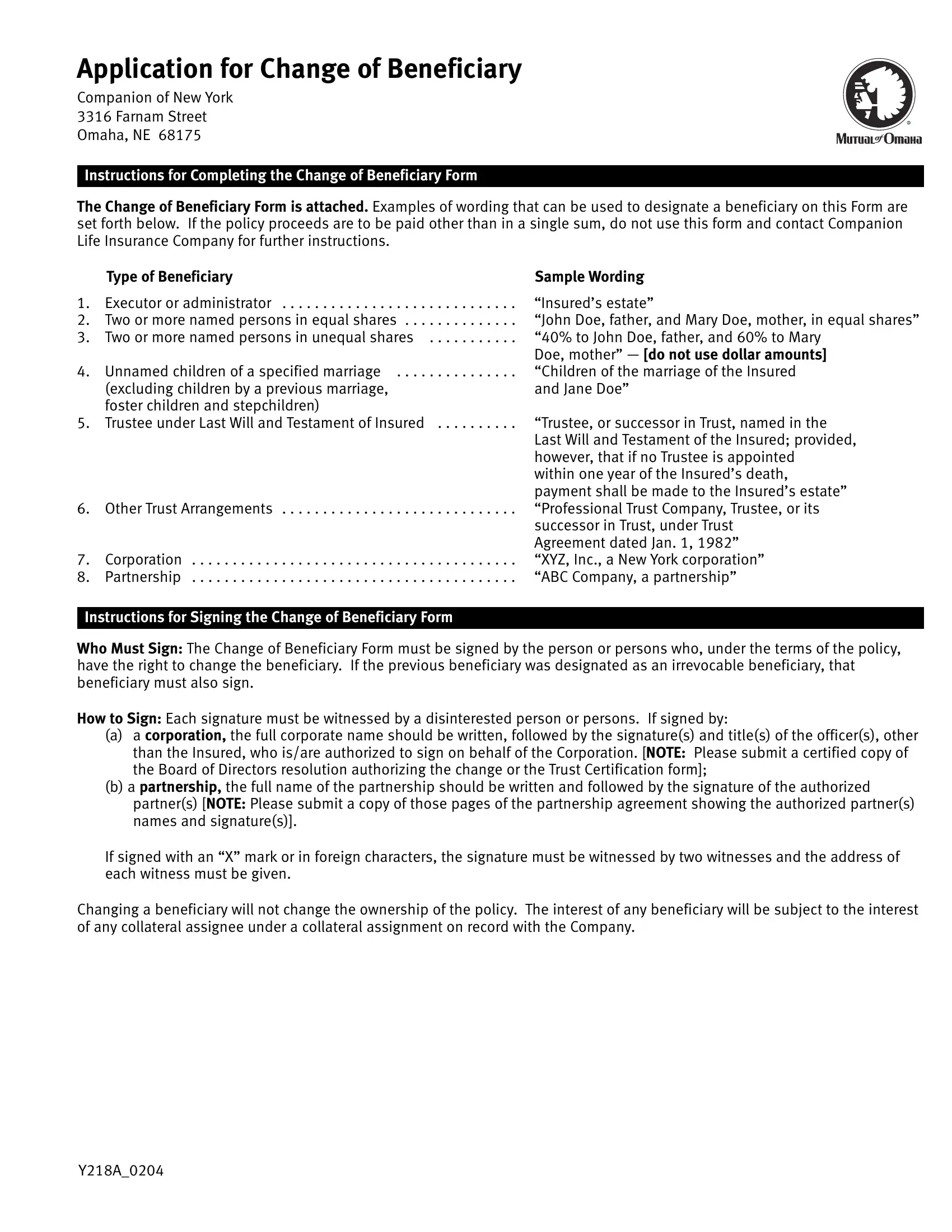
Application for Change of Beneficiary
Companion of New York
3316 Farnam Street
Omaha, NE 68175
Instructions for Completing the Change of Beneficiary Form
The Change of Beneficiary Form is attached. Examples of wording that can be used to designate a beneficiary on this Form are set forth below. If the policy proceeds are to be paid other than in a single sum, do not use this form and contact Companion Life Insurance Company for further instructions.
Type of Beneficiary
1. Executor or administrator . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2. Two or more named persons in equal shares . . . . . . . . . . . . . .
3. Two or more named persons in unequal shares . . . . . . . . . . .
4. Unnamed children of a specified marriage . . . . . . . . . . . . . . .
(excluding children by a previous marriage, foster children and stepchildren)
5. Trustee under Last Will and Testament of Insured . . . . . . . . . .
6. Other Trust Arrangements . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
7. Corporation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
8. Partnership . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Instructions for Signing the Change of Beneficiary Form
Sample Wording
“Insured’s estate”
“John Doe, father, and Mary Doe, mother, in equal shares” “40% to John Doe, father, and 60% to Mary
Doe, mother” — [do not use dollar amounts] “Children of the marriage of the Insured and Jane Doe”
“Trustee, or successor in Trust, named in the Last Will and Testament of the Insured; provided, however, that if no Trustee is appointed
within one year of the Insured’s death, payment shall be made to the Insured’s estate” “Professional Trust Company, Trustee, or its successor in Trust, under Trust
Agreement dated Jan. 1, 1982” “XYZ, Inc., a New York corporation” “ABC Company, a partnership”
Who Must Sign: The Change of Beneficiary Form must be signed by the person or persons who, under the terms of the policy, have the right to change the beneficiary. If the previous beneficiary was designated as an irrevocable beneficiary, that beneficiary must also sign.
How to Sign: Each signature must be witnessed by a disinterested person or persons. If signed by:
(a)a corporation, the full corporate name should be written, followed by the signature(s) and title(s) of the officer(s), other than the Insured, who is/are authorized to sign on behalf of the Corporation. [NOTE: Please submit a certified copy of the Board of Directors resolution authorizing the change or the Trust Certification form];
(b)a partnership, the full name of the partnership should be written and followed by the signature of the authorized partner(s) [NOTE: Please submit a copy of those pages of the partnership agreement showing the authorized partner(s) names and signature(s)].
If signed with an “X” mark or in foreign characters, the signature must be witnessed by two witnesses and the address of each witness must be given.
Changing a beneficiary will not change the ownership of the policy. The interest of any beneficiary will be subject to the interest of any collateral assignee under a collateral assignment on record with the Company.
Y218A_0204
Change of Beneficiary Form
Important!
1.Complete, sign and return this form for each Policy and/or Policy rider for which you are requesting a change.
2.Please use full given names (for example, “Mary E. Doe” and not “Mrs. John E. Doe”).
3.Do not send the Policy with this form unless we instruct you to do so.
4.Forms cannot be accepted which contain corrections or erasures.
Name ofPolicy
Insured: ___________________________________________________ Number: _________________________________________
As Policyowner, I hereby revoke any previous Beneficiary designation and election of settlement, I request that, on the death of the Insured named above, all proceeds of the Policy and/or rider(s) covering the named Insured be paid to the following beneficiary or beneficiaries as shown below:
Class |
Please Print |
Date of Birth |
Relationship to |
Percentage of |
|
Full Name and Address of Each Beneficiary |
|
Insured |
Proceeds Payable |
|
|
|
|
|
Primary |
|
|
|
|
Beneficiary(ies) |
|
|
|
|
|
|
|
|
|
Contingent |
|
|
|
|
(secondary) |
|
|
|
|
Beneficiary(ies) |
|
|
|
|
|
|
|
|
|
■Irrevocable Primary Beneficiary (ies): If this Box is checked, the Policy will be endorsed to show that the Primary Beneficiary (ies) named above is/are irrevocable. Changes to the Policy and/or rider(s), including a change of beneficiary (ies), may not be made by the Policyowner(s)/Trustee(s) without the consent of the Irrevocable Primary Beneficiary (ies) shown above.
Unless otherwise shown above: (a) payment will be shared equally by all Primary Beneficiaries who survive the Insured; if none, by all Contingent Beneficiaries who survive the Insured; (b) the right to change the beneficiary is reserved unless otherwise stated; (c) payment shall be made in a single sum; and (d) the word “child” or “children” shall include legally adopted children.
IT IS AGREED THAT THE INSTRUCTIONS APPEARING ON THE PRIOR PAGE ARE PART OF THIS CHANGE OF BENEFICIARY FORM.
The Company reserves the right to declare this form void and of no effect if it is incomplete or completed in an unsatisfactory manner.
Dated at ________________________________________________ this ___________ day of ___________________ , _________
City and State
( |
) |
|
_________________________________________________ |
||
Area Code |
Phone Number of Policyowner |
|
____________________________________________________
Signature of Policyowner(s)/Trustee(s) (If the Policyowner is a corporation or partnership, include authorized signature(s)
____________________________________________________
Signature of all Irrevocable Primary Beneficiary(ies) (if applicable) prior to submitting this Form
Mailing Directions (Please Print)
Return acknowledgment of change to:
__________________________________________________________
Name
__________________________________________________________
Address
__________________________________________________________
City |
State |
ZIP Code |
Is this a new mailing address? ■ Yes ■ No