Our PDF editor is designed to make completing official forms as straightforward as possible. Follow the steps below to fill out, edit, and download your Application Exemption form.
Step 1: Click the "Get Form" button to open the form in our online editor.
Step 2: Use the editing tools to fill in all required fields. You can add text, check boxes, insert signatures, highlight sections, and delete unused areas.
Complete the required fields in each part of the form:
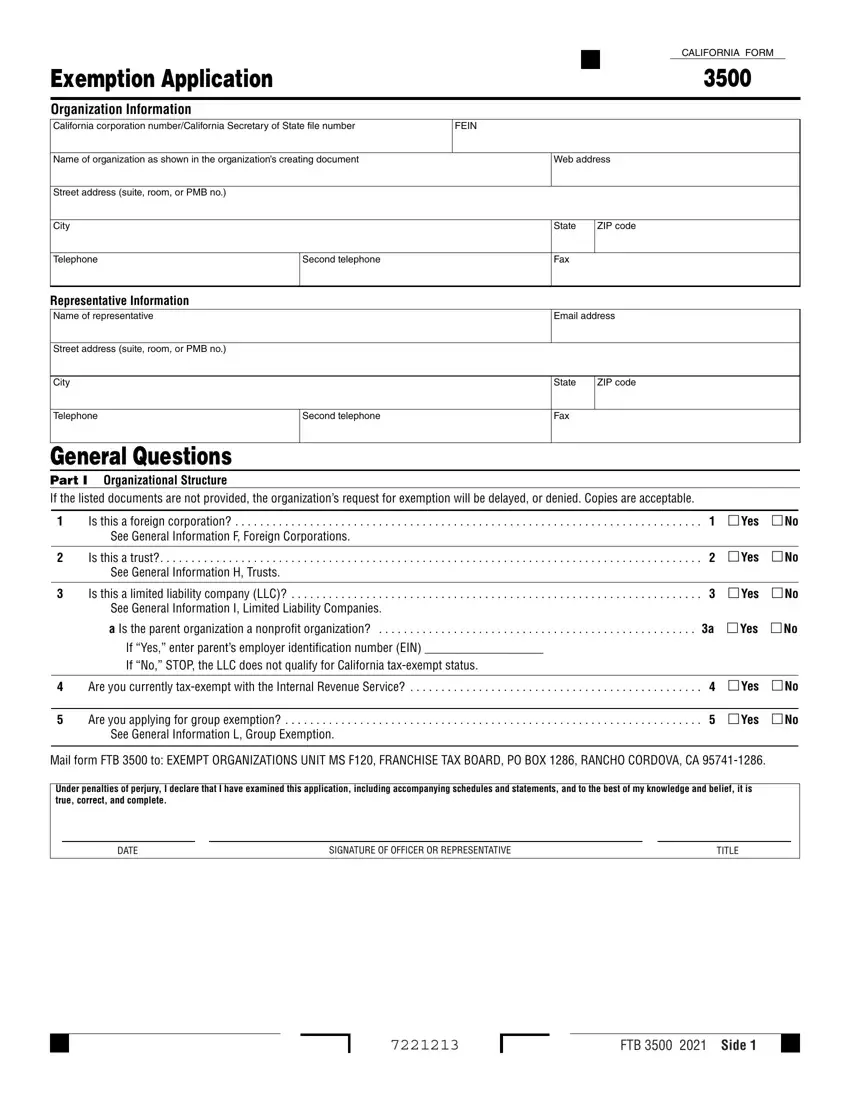
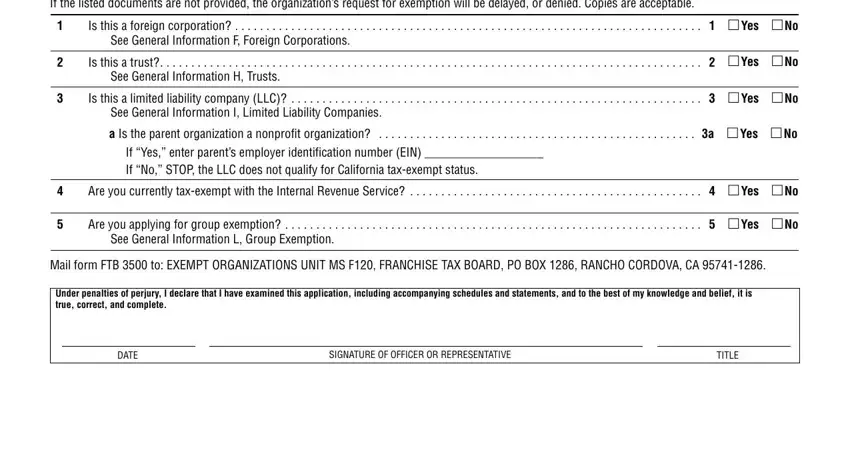
In Part I (General Questions), answer whether your organization is a foreign corporation, trust, or limited liability company. Indicate your current tax-exempt status with the IRS and whether you are applying for group exemption.
In Part II (Narrative of Activities), describe your organization’s activities, California connection, and annual revenue. Include the date the organization was formed and its primary purpose.
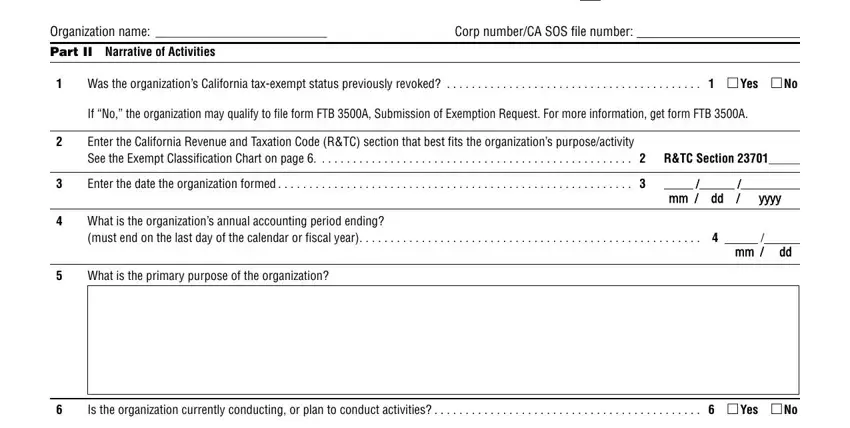
If your organization previously qualified for exemption, provide the date. If not, explain why it has not yet qualified.
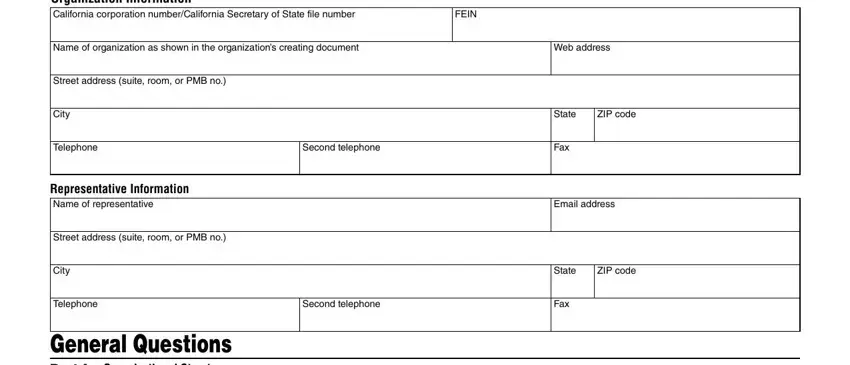
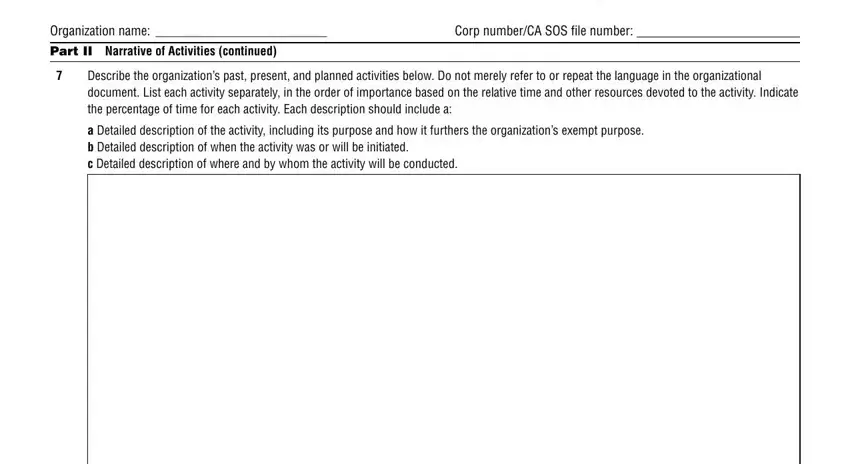
In the final section, provide your organization’s full name, corporate number (CA SOS file number), and a detailed description of past and planned activities.
Step 3: Click the "Done" button to save your completed form. The file is ready to download to your device.
Step 4: Save at least two copies of the completed form for your records before submitting to the California Franchise Tax Board.
Frequently Asked Questions
What is the Application Exemption form used for?
The Application Exemption form (California Form 3500) is used by organizations to apply for state income tax-exempt status with the California Franchise Tax Board. It is required for nonprofits, charitable foundations, and other qualifying organizations in California.
Who needs to file California Form 3500?
Nonprofit corporations, charitable organizations, religious groups, scientific institutions, and educational entities in California must file Form 3500 if they want exemption from California state income taxes. Organizations that already have IRS federal exempt status still need to apply separately at the state level.
How long does the review process take?
The California Franchise Tax Board typically processes applications within a few weeks to several months. Applications requiring additional documentation or clarification may take longer. Complete all required sections accurately to avoid unnecessary delays.
Can I submit the form online?
The California Franchise Tax Board accepts Form 3500 by mail. Use our free PDF editor to complete, sign, and print your form before mailing it to the FTB. This ensures all fields are filled in clearly and accurately.
Related Exemption Forms
Need to fill out a similar form? Browse these related exemption documents available on FormsPal:
- California Form 3500 - The official state tax exemption application worksheet for California organizations
- Texas Application Exemption - Tax exemption application for organizations based in Texas
- Homestead Exemption Application - Property tax exemption for qualifying homeowners
- Form ST-3 Tax Exemption - Sales tax exemption certificate for qualifying purchases
