
Use our free online PDF editor to complete the PeachCare for Kids application. Follow the steps below to fill out and download the form. No account or software download is required.
Step 1: Click the orange "Get Form" button above to open the application in the PDF editor. Follow the prompts on screen to navigate to the form.
Step 2: The editor lets you type text, add signatures, and make corrections to the main application form. You can skip any section that does not apply to your household's situation.
Complete every required field carefully. Incomplete or inaccurate information may delay the application review.
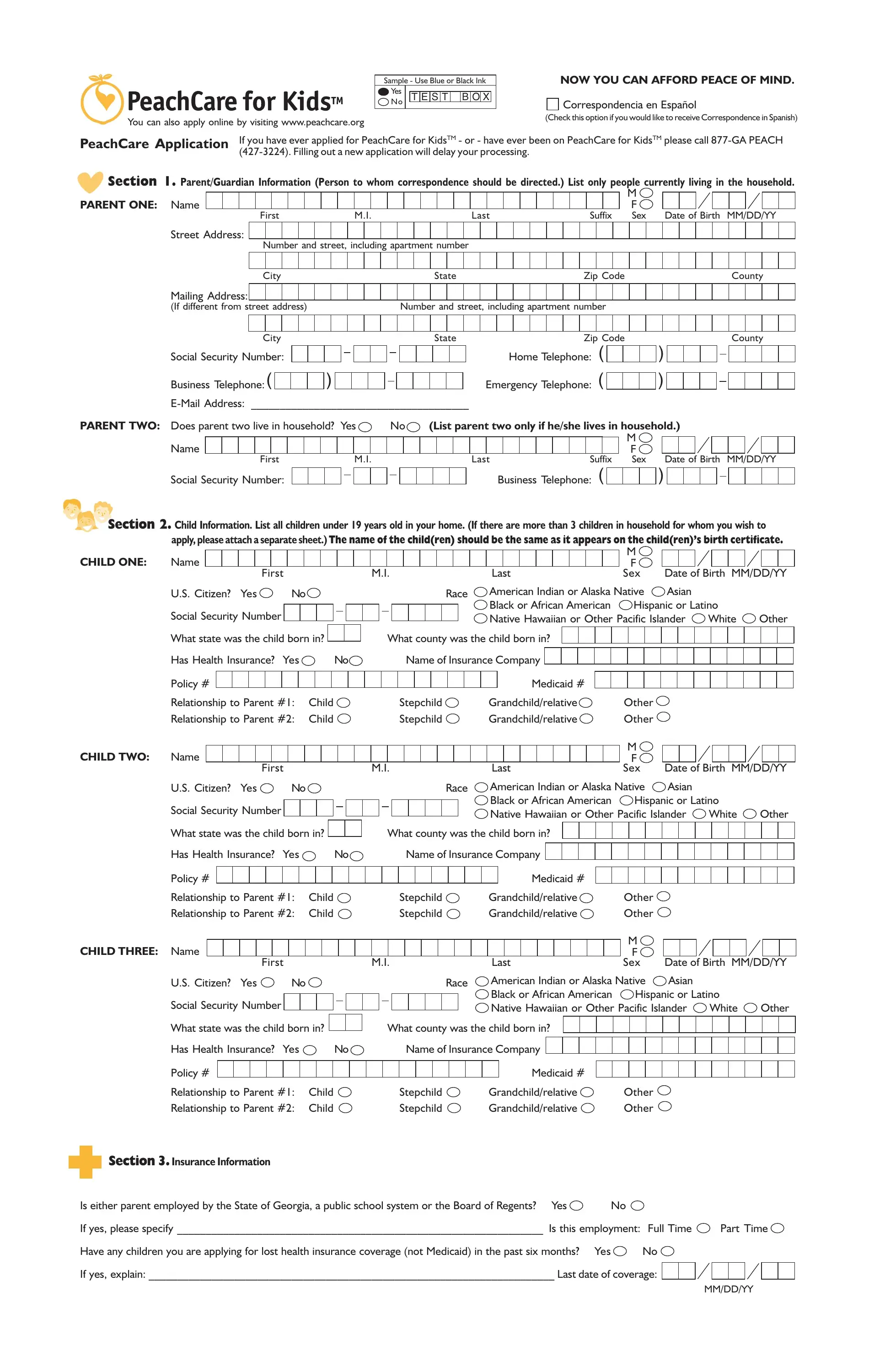
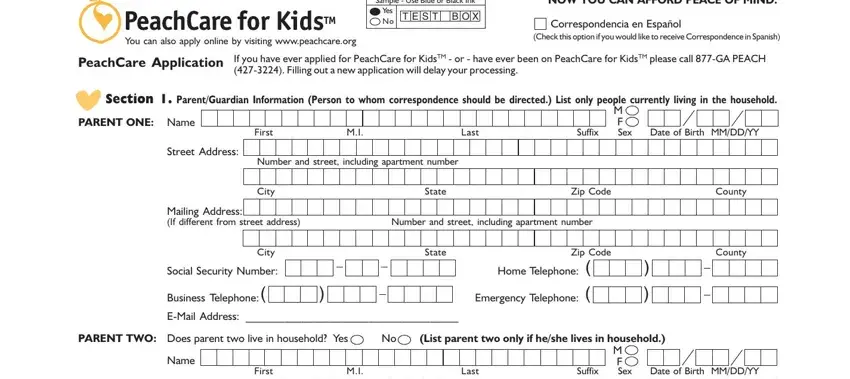
1. Start with the parent or guardian identification section. Enter your full name, home address, Social Security Number, and phone number.
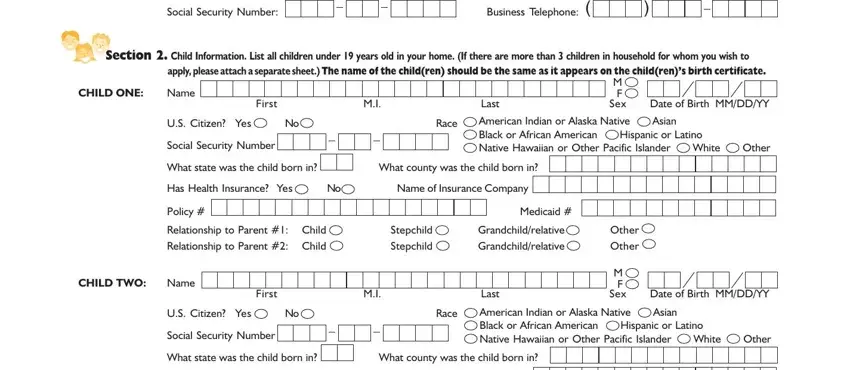
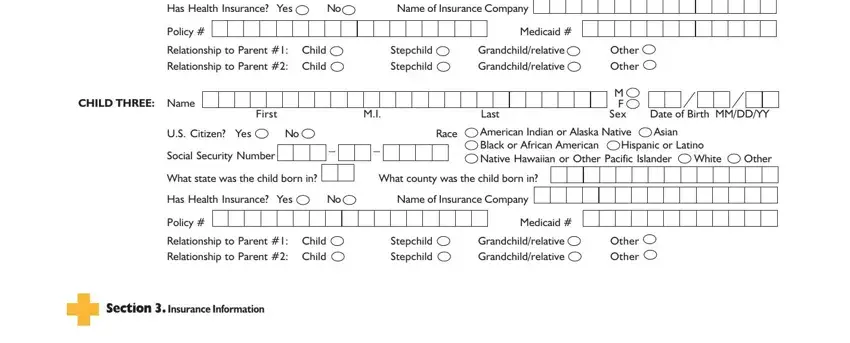
2. In the Child Information section, enter each child's first and last name, date of birth, sex, Social Security Number, U.S. citizenship status, and race. Indicate whether any child already has health coverage.
3. The insurance section asks about existing health coverage for the children. List the name of the insurance company, the policy number, and how each child is related to the policyholder. If a child has Medicaid, note that in this section as well.
4. For the employment section, indicate whether either parent is currently employed. If employment changed recently, note the last date of work and the reason for the change.
5. In the income section, list all household income: wages, self-employment earnings, Social Security payments, child support, unemployment benefits, retirement income, and any other sources. Attach proof of income documents with your completed application.
Step 3: After completing all sections, click "Done" to save your application. Download, print, or submit the form directly. For related medical assistance forms, see the Georgia Medicaid application or the health insurance application.
FormsPal keeps your information private. All data entered in our editor is kept confidential and not shared with third parties.