
Handling PDF forms online is always simple using our PDF tool. Anyone can fill out the ARIS Solutions Employee Packet here in a matter of minutes. FormsPal is focused on making sure you have the absolute best experience with our tool by constantly adding new functions and improvements. With all of these improvements, working with our editor becomes better than ever. Should you be seeking to get started, here is what it takes:
Step 1: Click the "Get Form" button above. It will open our PDF tool so that you can start completing your form.
Step 2: This tool will allow you to customize your PDF file in a variety of ways. Improve it with your own text, correct what is originally in the PDF, and include a signature - all at your convenience!
Completing this form requires careful attention to detail. Ensure that all mandatory blank fields are filled out correctly.
1. It is crucial to fill out the ARIS Solutions Employee Packet correctly, so be careful while filling in the segments comprising these blank fields:

Step 3: Before moving on, you should make sure that blanks were filled out right. As soon as you are satisfied with it, press "Done." Create a 7-day free trial option at FormsPal and obtain direct access to the ARIS Solutions Employee Packet - download, email, or edit from your personal account. When you use FormsPal, you can easily complete documents without stressing about information breaches or entries getting shared. Our protected system helps to ensure that your personal data is maintained safely.
Key Sections in the ARIS Solutions Employee Packet
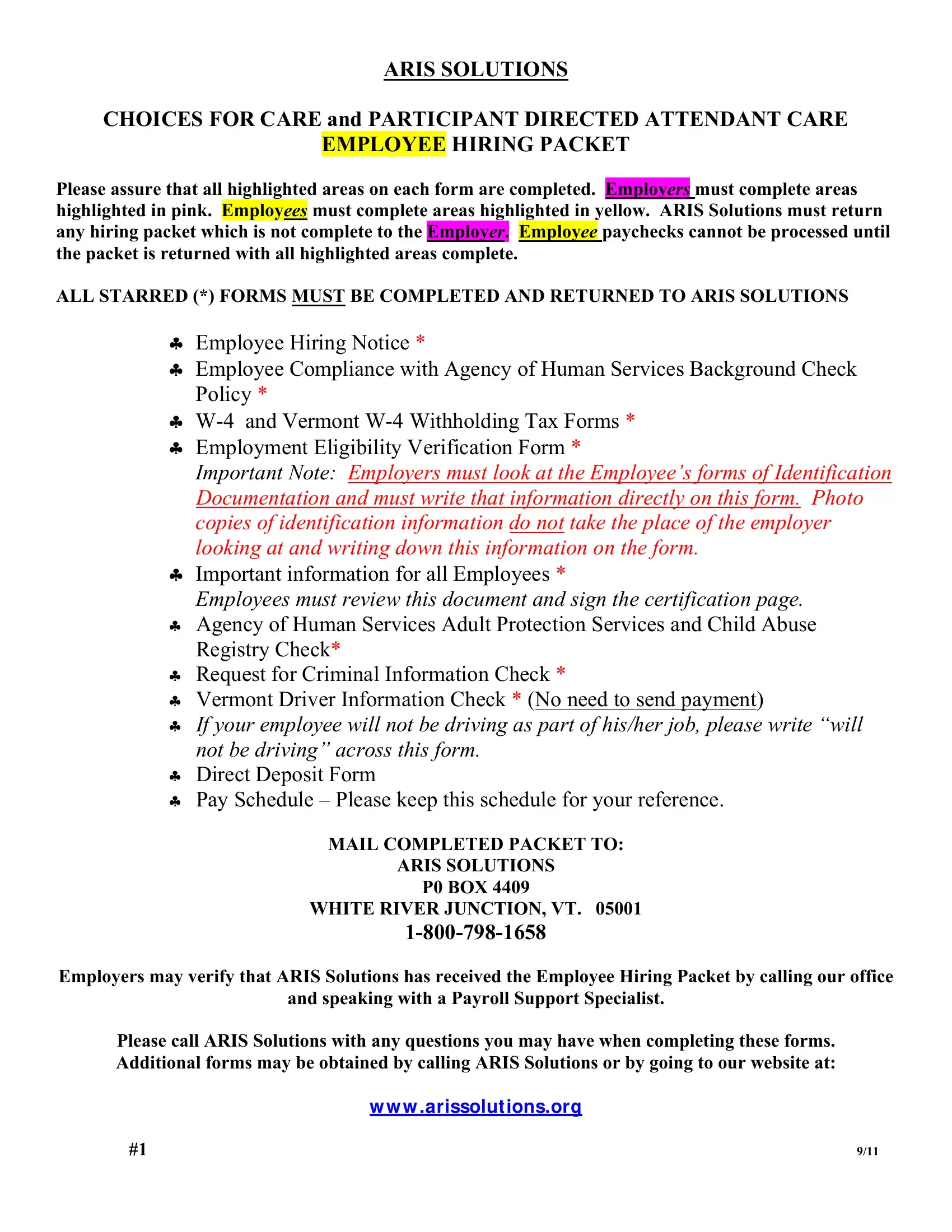
The packet contains several critical forms that both employers and employees must complete before ARIS Solutions can process payroll:
- Employee Hiring Notice - Review the employment terms and confirm the start date and job responsibilities before signing.
- W-4 and Vermont W-4 Withholding Tax Forms - Declare your federal and state income tax withholding preferences. These figures affect every paycheck you receive.
- Employment Eligibility Verification (I-9) - Confirm your legal right to work in the United States. Have valid identity documents ready when completing this section.
- Background Check Authorization - Required by the Agency of Human Services for all participants in Vermont's Choices for Care and Attendant Care programs.
- Direct Deposit Form - Provide your bank routing number and account number for payroll direct deposit setup.
Common Mistakes When Completing the ARIS Solutions Employee Packet
Avoid these frequent errors to prevent delays in paycheck processing:
- Leaving required fields blank on the W-4 or Vermont W-4 forms.
- Forgetting to sign and date the Background Check authorization page.
- Using outdated form versions - always confirm you have the current packet from ARIS Solutions.
- Skipping the Direct Deposit form, which delays your first paycheck.
- Misidentifying which sections apply to employers versus employees. Pink-highlighted fields are for employers and yellow-highlighted fields are for employees.
For additional employment and payroll documents, browse FormsPal's employment forms library or review our caregiver daily log template for tracking work hours under the Attendant Care program.