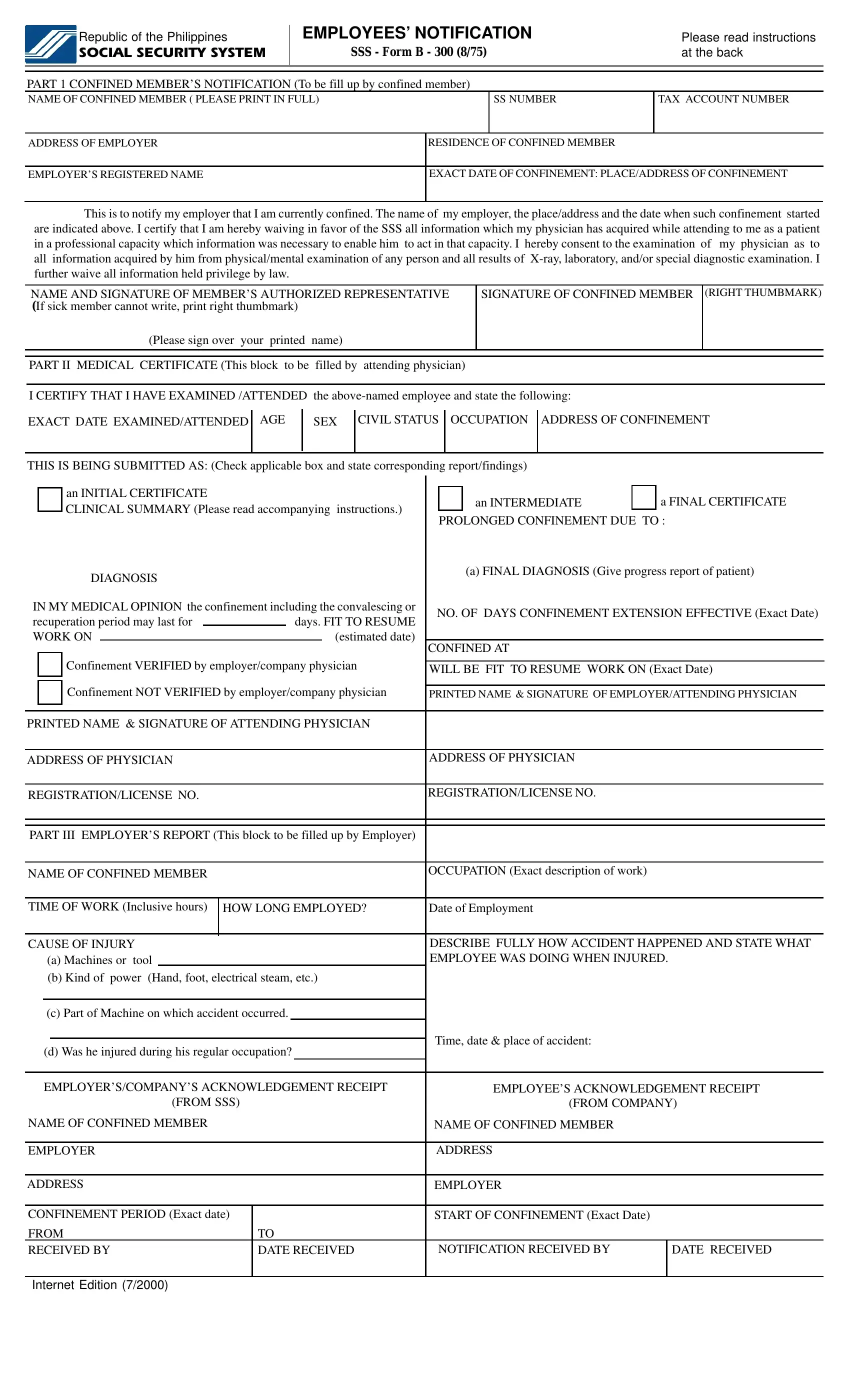
In the realm of workplace health management and social security within the Philippines, the Social Security System (SSS) Employee Notification form emerges as a critical document, designed to streamline the process of reporting employee sickness or injury. The comprehensive form, known as SSS Form B-300, serves multiple purposes: it facilitates communication between the confined employee and their employer, ensures the attending physician's findings are systematically recorded, and aids the Social Security System in evaluating and processing confinement-related benefits. The form is methodically divided into three distinct parts -- the confined member’s notification, a medical certificate, and the employer’s report -- each requiring specific details to be filled out by the respective stakeholders. This seamless integration of information gathering and submission requirements underscores the form’s significance in expediting the issuance of benefits, while also emphasizing the importance of timely and thorough communication among all parties involved. Moreover, it embodies the procedural legwork necessary for an employee to officially notify their employer and the SSS about their confinement, waiving physician-patient privacy to the extent needed for benefit processing, and laying down the groundwork for assessing the duration of leave and fitness to resume work. The detailed instructions accompanying the form ensure clarity and compliance, highlighting the critical timelines and documentation essential for a smooth benefit claim process.
| Question | Answer |
|---|---|
| Form Name | Sss Employee Notification Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | sss sickness notification form, sss form b300 pdf, sss form b 300, b300 sss form |
