
Dealing with PDF forms online is a piece of cake with this PDF editor. Anyone can fill out Arkansas Name Change Request Form here in a matter of minutes. Our team is constantly endeavoring to improve the editor and insure that it is much better for people with its multiple functions. Capitalize on present-day innovative possibilities, and find a trove of emerging experiences! With just a couple of basic steps, you are able to begin your PDF editing:
Step 1: Simply click the "Get Form Button" at the top of this site to see our pdf file editor. There you'll find everything that is needed to work with your file.
Step 2: The tool grants the opportunity to modify your PDF in a variety of ways. Modify it with personalized text, adjust what's already in the document, and include a signature - all when you need it!
This document will require particular details to be entered, so make sure you take whatever time to fill in what is expected:
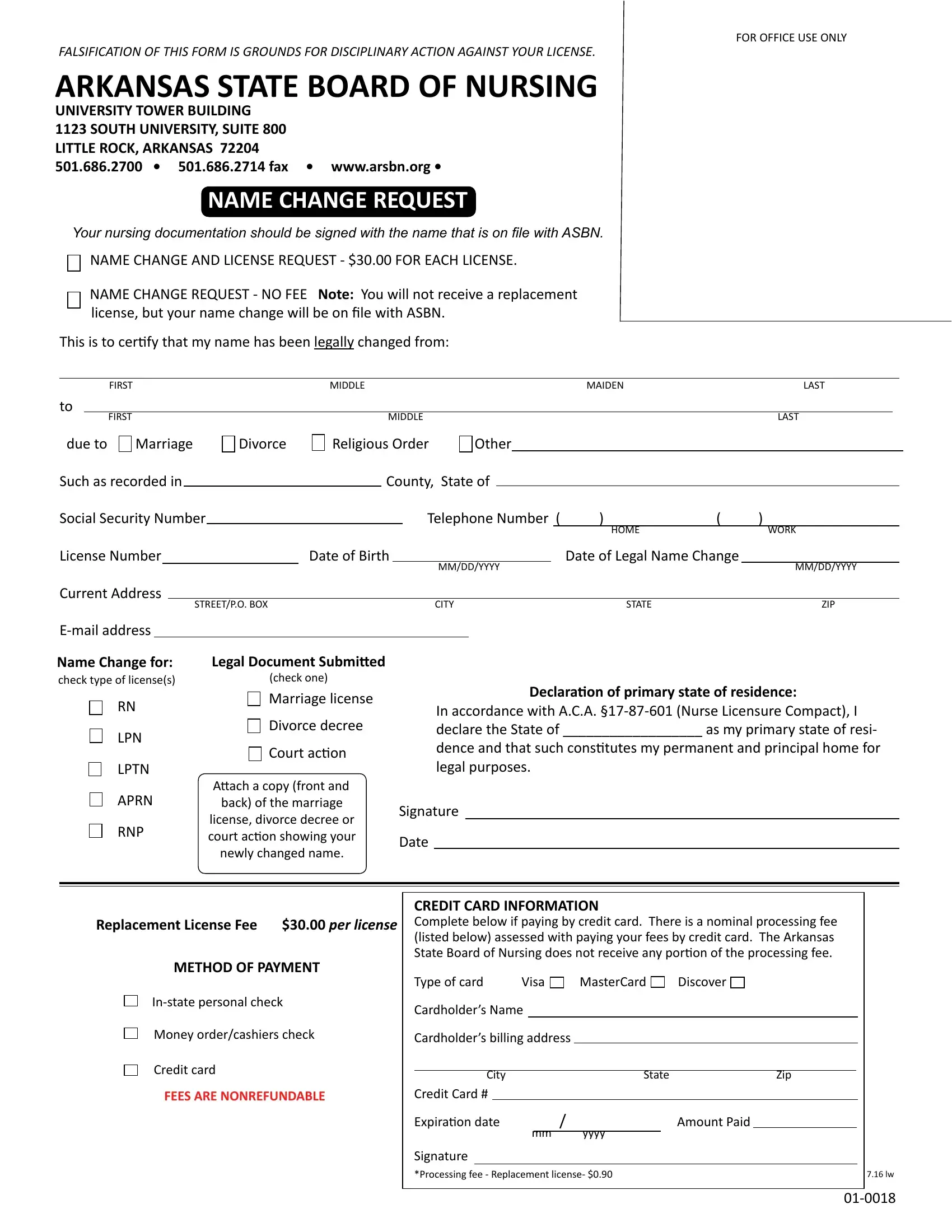
1. To get started, while filling out the Arkansas Name Change Request Form, beging with the area that has the next fields:
2. When the prior section is completed, proceed to enter the relevant details in all these - LPTN, APRN, RNP, Divorce decree Court action, Attach a copy front and back of, license divorce decree or court, newly changed name, In accordance with ACA Nurse, Signature, Date, Replacement License Fee per, METHOD OF PAYMENT, Instate personal check, Money ordercashiers check, and Credit card.
People who use this PDF often make some mistakes when filling in Attach a copy front and back of in this section. Ensure you read twice whatever you enter here.
Step 3: Soon after taking one more look at your fields you've filled in, hit "Done" and you're done and dusted! Make a 7-day free trial option at FormsPal and gain immediate access to Arkansas Name Change Request Form - which you are able to then work with as you would like from your personal account page. We don't share or sell any details you provide whenever completing forms at our site.