Navigating through the complexities of healthcare compliance requires a thorough understanding of various regulatory requirements, including the process of submitting an Attestation Sample form for provider-based status. This form serves as a crucial component for healthcare facilities seeking to establish or maintain their provider-based status under Centers for Medicare & Medicaid Services (CMS) guidelines. Specifically designed to illustrate compliance with the stringent criteria set forth in 42 CFR 413.65, the document outlines detailed requirements across multiple aspects, such as the physical and financial integration of the main provider and the facility, adherence to state and federal regulations, and clear delineations of services provided. Facilities ranging from hospitals to specific exclusions like ambulatory surgical centers and independent diagnostic testing facilities are addressed, pinpointing the intricate scope of healthcare entities affected. Critical Access Hospitals (CAHs), along with Federally Qualified Health Centers (FQHCs) and Rural Health Clinics (RHCs), find themselves navigating distinct paths within these regulations, underscored by the significant implications of provider-based status on reimbursement rates and regulatory compliance. The Attestation Sample form mandates detailed provision of information including but not limited to operational, clinical, and financial integrations, further emphasizing the comprehensive nature of the CMS’s review process. Completing and submitting this form correctly is pivotal for healthcare providers aiming to affirm their provider-based status, directly influencing their operational legitimacy and financial landscape within the Medicare program.
| Question | Answer |
|---|---|
| Form Name | Attestation Form Sample |
| Form Length | 9 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min 15 sec |
| Other names | attestation form filled sample, filled attestation form sample, attestation how fill, printable attestation forms |
Exhibit 1 |
1 |
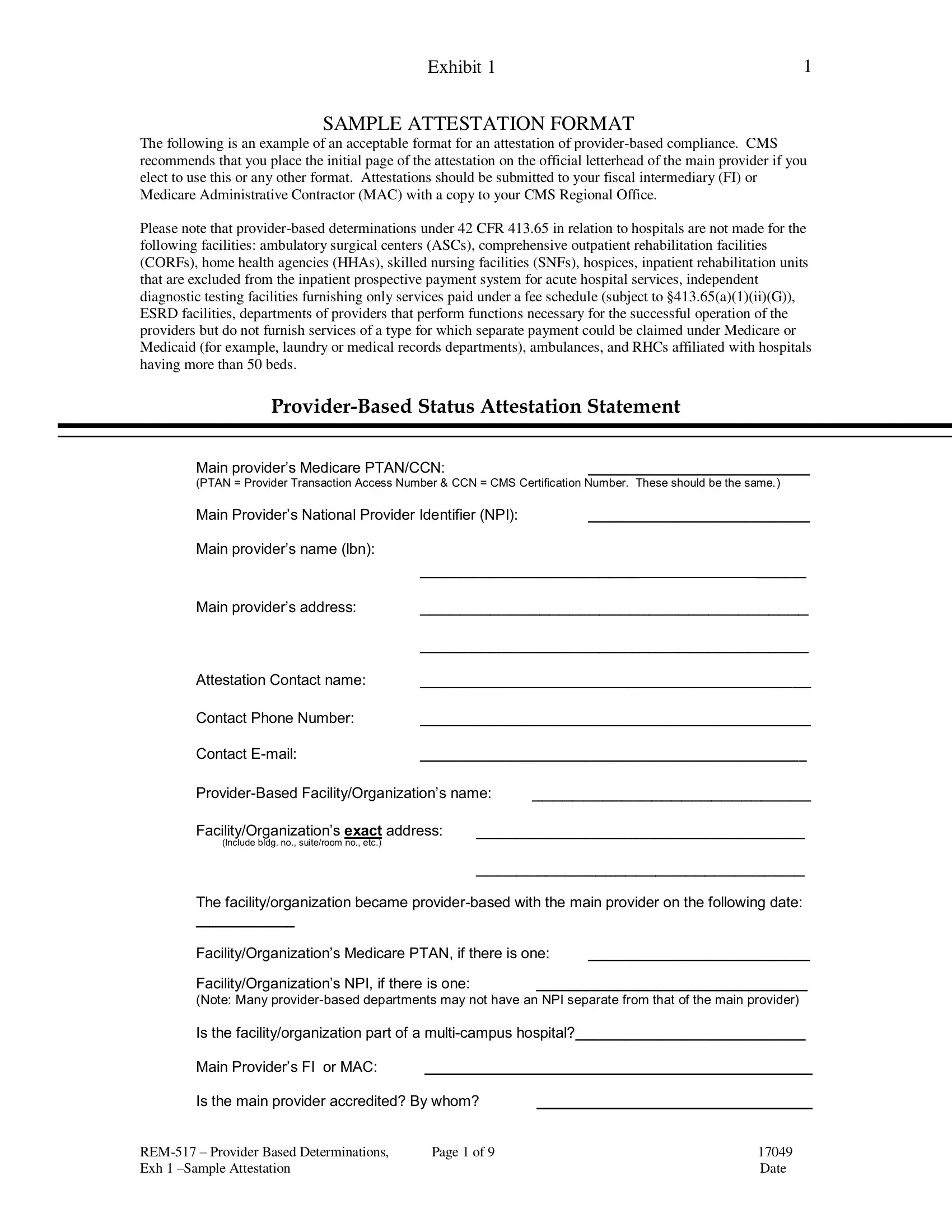
SAMPLE ATTESTATION FORMAT
The following is an example of an acceptable format for an attestation of
Please note that
Main provider’s Medicare PTAN/CCN: |
___________________________ |
(PTAN = Provider Transaction Access Number & CCN = CMS Certification Number. These should be the same.)
Main Provider’s National Provider Identifier (NPI): |
___________________________ |
||||
Main provider’s name (lbn): |
|
|
|
|
|
|
______________________ |
|
_____ |
||
Main provider’s address: |
_______________________________________ |
||||
|
_______________________________________ |
||||
Attestation Contact name: |
___________________________________________ |
||||
Contact Phone Number: |
___________________________________________ |
||||
Contact |
_______________________________________________ |
||||
____________________________ |
|||||
Facility/Organization’s exact address: |
_________________________________ |
||||
(Include bldg. no., suite/room no., etc.) |
|
|
|
|
|
_________________________________
The facility/organization became
____________
Facility/Organization’s Medicare PTAN, if there is one: |
___________________________ |
|
Facility/Organization’s NPI, if there is one: |
_________________________________ |
|
(Note: Many
Is the facility/organization part of a
Main Provider’s FI or MAC:
Is the main provider accredited? By whom?
Page 1 of 9 |
17049 |
|
Exh 1 |
|
Date |
Exhibit 1 |
|
2 |
|
For Critical Access Hospitals |
|
|
|
Is the main provider a critical access hospital (CAH)? |
Y |
N |
|
If so, please read and certify the following: |
|
|
|
There are now prohibitions against the acquisition or creation of
Please complete A OR B below:
A._________ This facility satisfies the requirements of 42 CFR §485.610(e) because (please check all that apply):
______ It is an RHC,
January 1, 2008.
______ It is located more than a
terrain or in areas with only secondary roads available, a
______ This facility was “under development” prior to January 1, 2008. (Please
include a copy of the letter from the CMS Regional Office recognizing that plans existed prior to January 1, 2008, for the CAH to acquire or construct the provider- based facility or distinct part unit.)
B._________ I understand that the facility does not meet the provisions of
42 CFR §485.610(e) and wish to attest to the
further understand that treatment of this facility as
For Other Entities: |
|
Is the facility a Federally Qualified Health Center (FQHC)? Y |
N |
If so, and if the FQHC meets the criteria at section 413.65(n), it need not attest to its provider- based status. The
Is the facility a Rural Health Clinic (RHC)?Y N
If so, Medicare will not make a
Page 2 of 9 |
17049 |
|
Exh 1 |
|
Date |

Exhibit 1 |
3 |
Please indicate if this attestation is adding, deleting, or changing previously submitted attestation information, including the effective date:
Add |
|
Delete |
|
Change |
Effective Date |
Please indicate the types of services furnished at the facility (please check all that apply):
1.Outpatient hospital services and supplies incident to a physician service
2.Outpatient hospital diagnostic services
3.Outpatient hospital therapy services, including any combination of occupational therapy, physical therapy, and/or
4.Other (please specify)
I certify that I have carefully read the attached sections of the Federal
1._____ The facility/organization is “on campus” per 42 C.F.R. §413.65(a)(2) and is in compliance with the following
OR
2._____ The facility/organization is “off campus” per 42 C.F.R. §413.65(a)(2) and is in compliance with the following
If the
Page 3 of 9 |
17049 |
|
Exh 1 |
|
Date |
Exhibit 1 |
4 |
Please complete the following for on campus AND off campus facilities and organizations:
I attest that the facility/organization complies with the following requirements to be provider- based to the main provider (please indicate Yes or No for each requirement):
1.____ The department of the provider, the remote location of a hospital, or the satellite facility and the main provider are operated under the same license, except in areas where the State requires a separate license for the department of the provider, the remote location of a hospital, or the satellite facility, or in States where State law does not permit licensure of the provider and the prospective department of the provider, the remote location of a hospital, or
the satellite facility under a single license. If the provider and facility/organization are located in a state having a health facilities’ cost review commission or other agency that has authority to regulate the rates charged by hospitals or other providers, the commission or agency has not found that the facility/organization is not part of the provider.
2.____ The clinical services of the facility or organization seeking
2a. ____ Professional staff of the facility or organization have clinical privileges at the
main provider.
2b. ____ The main provider maintains the same monitoring and oversight of the facility or
organization as it does for any other department of the provider.
2c. ____ The medical director of the facility or organization seeking
maintains a reporting relationship with the chief medical officer or other similar official of the main provider that has the same frequency, intensity, and level of accountability that exists in the relationship between the medical director of a department of the main provider and the chief medical officer or other similar official of the main provider, and is under the same type of supervision and accountability as any other director, medical or otherwise, of the main provider.
2d. ____ Medical staff committees or other professional committees at the main provider are
responsible for medical activities in the facility or organization, including quality assurance, utilization review, and the coordination and integration of services, to the extent practicable, between the facility or organization seeking
2e. ____ Medical records for patients treated in the facility or organization are integrated into
a unified retrieval system (or cross reference) of the main provider.
2f. ____ Inpatient and outpatient services of the facility or organization and the main provider
are integrated, and patients treated at the facility or organization who require further care have full access to all services of the main provider and are referred where appropriate to the corresponding inpatient or outpatient department or service of the main provider.
3.____ The financial operations of the facility or organization are fully integrated within the financial system of the main provider, as evidenced by shared income and expenses between the main provider and the facility or organization. The costs of a facility or organization that is a hospital department are reported in a cost center of the provider, costs of a
any
Page 4 of 9 |
17049 |
|
Exh 1 |
|
Date |
Exhibit 1 |
5 |
4.____ The facility or organization seeking status as a department of a provider, a remote location of a hospital, or a satellite facility is held out to the public and other payers as part of the main provider. When patients enter the
5.____ In the case of a hospital outpatient department or a
5a. ____ Hospital outpatient departments located either on or off the campus of the hospital
that is the main provider comply with the
(r) and §489.24 of chapter IV of Title 42.
5b. ____ Physician services furnished in hospital outpatient departments or
entities (other than RHCs) are billed with the correct
5c. ____ Hospital outpatient departments comply with all the terms of the hospital’s provider
agreement.
5d. ____ Physicians who work in hospital outpatient departments or
comply with the
5e. ____ Hospital outpatient departments (other than RHCs) treat all Medicare patients, for
billing purposes, as hospital outpatients. The departments do not treat some Medicare patients as hospital outpatients and others as physician office patients.
5f. ____ In the case of a patient admitted to the hospital as an inpatient after receiving
treatment in the hospital outpatient department or
413.40(c)(2) of chapter IV of Title 42, respectively. (Note: If the potential main provider is a CAH, enter “NA” for this item).
5g. ____ (Note: This requirement only applies to off campus facilities. This obligation
does not apply to services where there is no professional component to the hospital’s technical component charge, e.g laboratory, Physical Therapy,
Occupational Therapy, and Speech Pathology services). When a Medicare
beneficiary is treated in a hospital outpatient department or
not required to be provided by the antidumping rules in §489.24 of chapter IV of Title
42, the hospital provides written notice to the beneficiary, before the delivery of services, of the amount of the beneficiary’s potential financial liability (that is, that the
beneficiary will incur a coinsurance liability for an outpatient visit to the hospital as well as for the physician service, and of the amount of that liability).
(1)____The notice is on that the beneficiary can read and understand.
(2)____If the exact type and extent of care needed is not known, the hospital furnishes
a written notice to the patient that explains that the beneficiary will incur a coinsurance liability to the hospital that he or she would not incur if the facility were not provider-
based, AND the hospital furnishes an estimate based on typical or average charges for visits to the facility, but states that the patient’s actual liability will depend upon the
actual services furnished by the hospital.
Page 5 of 9 |
17049 |
|
Exh 1 |
|
Date |
Exhibit 1 |
6 |
(3)____If the beneficiary is unconscious, under great duress, or for any other reason is |
|
unable to read a written notice and understand and act on his or her own rights, the |
|
notice is provided before the delivery of services, to the beneficiary’s authorized |
|
representative. |
|
(4)____In cases where a hospital outpatient department provides examination or |
|
treatment that is required to be provided by the antidumping rules at § 489.24 of |
|
chapter IV of Title 42, the notice is given as soon as possible after the existence of an |
|
emergency condition has been ruled out or the emergency condition has been |
|
stabilized. |
|
5h. _____ Hospital outpatient departments meet applicable hospital health and safety rules for
Please include a copy of your Medicare beneficiary coinsurance notice and a copy of the provider’s policy and procedures for completion of the notice as documentation for this
obligation of
For
In addition to the above requirements (numbers
6.____ The facility or organization seeking
6a. _____ The business enterprise that constitutes the facility or organization is 100 percent
owned by the provider.
6b. ____ The main provider and the facility or organization seeking status as a department of
the provider, a remote location of a hospital, or a satellite facility have the same governing body.
6c. ____ The facility or organization is operated under the same organizational documents as
the main provider. For example, the facility or organization seeking
6d. _____ The main provider has final responsibility for administrative decisions, final
approval for contracts with outside parties, final approval for personnel actions, final responsibility for personnel policies (such as fringe benefits or code of conduct), and final approval for medical staff appointments in the facility or organization.
7._____ The reporting relationship between the facility or organization seeking
7a. ____ The facility or organization is under the direct supervision of the main provider.
7b. ____ The facility or organization is operated under the same monitoring and oversight by
the provider as any other department of the provider, and is operated just as any other department of the provider with regard to supervision and accountability. The facility or organization director or individual responsible for daily operations at the
Page 6 of 9 |
17049 |
|
Exh 1 |
|
Date |
Exhibit 1 |
7 |
(1)____ Maintains a reporting relationship with a manager at the main provider that has the same frequency, intensity, and level of accountability that exists in the relationship between the main provider and its existing departments; and
(2)____ Is accountable to the governing body of the main provider, in the same manner as any department head of the provider.
7c. ____ The following administrative functions of the facility or organization are integrated
with those of the provider where the facility or organization is based: billing services, records, human resources, payroll, employee benefit package, salary structure, and purchasing services. Either the same employees or group of employees handle these administrative functions for the facility or organization and the main provider, or the administrative functions for both the facility or organization and the entity are (1) contracted out under the same contract agreement; or (2) handled under different contract agreements, with the contract of the facility or organization being managed by the main provider.
8._____ The facility or organization is located within a
8a. ____ The facility or organization is owned and operated by a hospital or CAH that has a
disproportionate share adjustment (as determined under §412.106 of chapter IV of Title
42)greater than 11.75 percent or is described in §412.106(c)(2) of chapter IV of Title 42 implementing section 1886(e)(5)(F)(i)(II) of the Act and is:
(1)____ Owned or operated by a unit of State or local government;
(2)____ A public or nonprofit corporation that is formally granted governmental powers by a unit of State or local government; or
(3)____ A private hospital that has a contract with a State or local government that includes the operation of clinics located off the main campus of the hospital to assure access in a
8b. ____ The facility or organization demonstrates a high level of integration with the main
provider by showing that it meets all of the other
(1)____ At least 75 percent of the patients served by the facility or organization reside in the same zip code areas as at least 75 percent of the patients served by the main provider;
(2)____ At least 75 percent of the patients served by the facility or organization who required the type of care furnished by the main provider received that care from that provider (for example, at least 75 percent of the patients of an RHC seeking
(3)____ If the facility or organization is unable to meet the criteria in (1) or (2) directly above because it was not in operation during all of the
Page 7 of 9 |
17049 |
|
Exh 1 |
|
Date |
Exhibit 1 |
8 |
8c. ____ If the facility or organization is attempting to qualify for
this section, then the facility or organization and the main provider are located in the same State or, when consistent with the laws of both States, in adjacent States.
Note: An RHC that is otherwise qualified as a
9.____ The facility or organization that is not located on the campus of the potential main provider and otherwise meets the requirements of
management contract, meets all of the following criteria (please respond to 9a - 9d if the facility is operated under a management contract; otherwise record “NA” for “not applicable”):
9a. ____ The main provider (or an organization that also employs the staff of the main
provider and that is not the management company) employs the staff of the facility or organization who are directly involved in the delivery of patient care, except for management staff and staff who furnish patient care services of a type that would be paid for by Medicare under a fee schedule established by regulations at Part 414 of
chapter IV of Title 42. Other than staff that may be paid under such a Medicare fee schedule, the main provider does not utilize the services of “leased'' employees (that is,
personnel who are actually employed by the management company but provide services for the provider under a staff leasing or similar agreement) that are directly involved in the delivery of patient care.
9b. ____ The administrative functions of the facility or organization are integrated with those
of the main provider, as determined under criteria in paragraph 7c above.
9c. ____ The main provider has significant control over the operations of the facility or
organization as determined under criteria in paragraph 7b above.
9d. ____ The management contract is held by the main provider itself, not by a parent
organization that has control over both the main provider and the facility or organization.
For facilities/organizations operated as joint ventures requesting
10.____ The facility or organization being attested to as
10a. ____ The facility is partially owned by at least one provider;
10b. ____ The facility is located on the main campus of a provider who is a partial owner;
10c. ____ The facility is
facility organization is located; and
10d. _____ The facility or organization meets all the requirements applicable to all
Page 8 of 9 |
17049 |
|
Exh 1 |
|
Date |

Exhibit 1 |
9 |
*I certify that the responses in this attestation and information in the documents are accurate, complete, and current as of this date. I acknowledge that the regulations must be continually adhered to. Any material change in the relationship between the facility/organization and the main provider, such as a change of ownership or entry into
a new or different management contract, may be reported to CMS. (NOTE: ORIGINAL ink signature must be submitted. Attestation must be signed by an official to whom the organization has granted the legal authority to commit the provider to fully abide by the statutes, regulations, and program instructions of the Medicare program.)
Signed:__________________________________________
(Signature of Officer or Administrator or authorized person)
__________________________
(PRINT Name of signature)
Title :___________________________________________
(Title of authorized person acting on behalf of the provider)
__________________________
(Direct telephone number)
Date :__________________________________________
*Whoever, in any matter within the jurisdiction of any department or agency of the United States knowingly and willfully falsifies, conceals or covers up by any trick, scheme or device a material fact, or makes any false, fictitious or fraudulent statement or representations, or makes or uses any false writing or document knowing the same to contain any false, fictitious or fraudulent statement or entry, shall be fined not more than $10,000 or imprisoned not more than five years or both. (18 U.S.C. § 1001).
Published: March 15, 2012
Page 9 of 9 |
17049 |
|
Exh 1 |
|
Date |