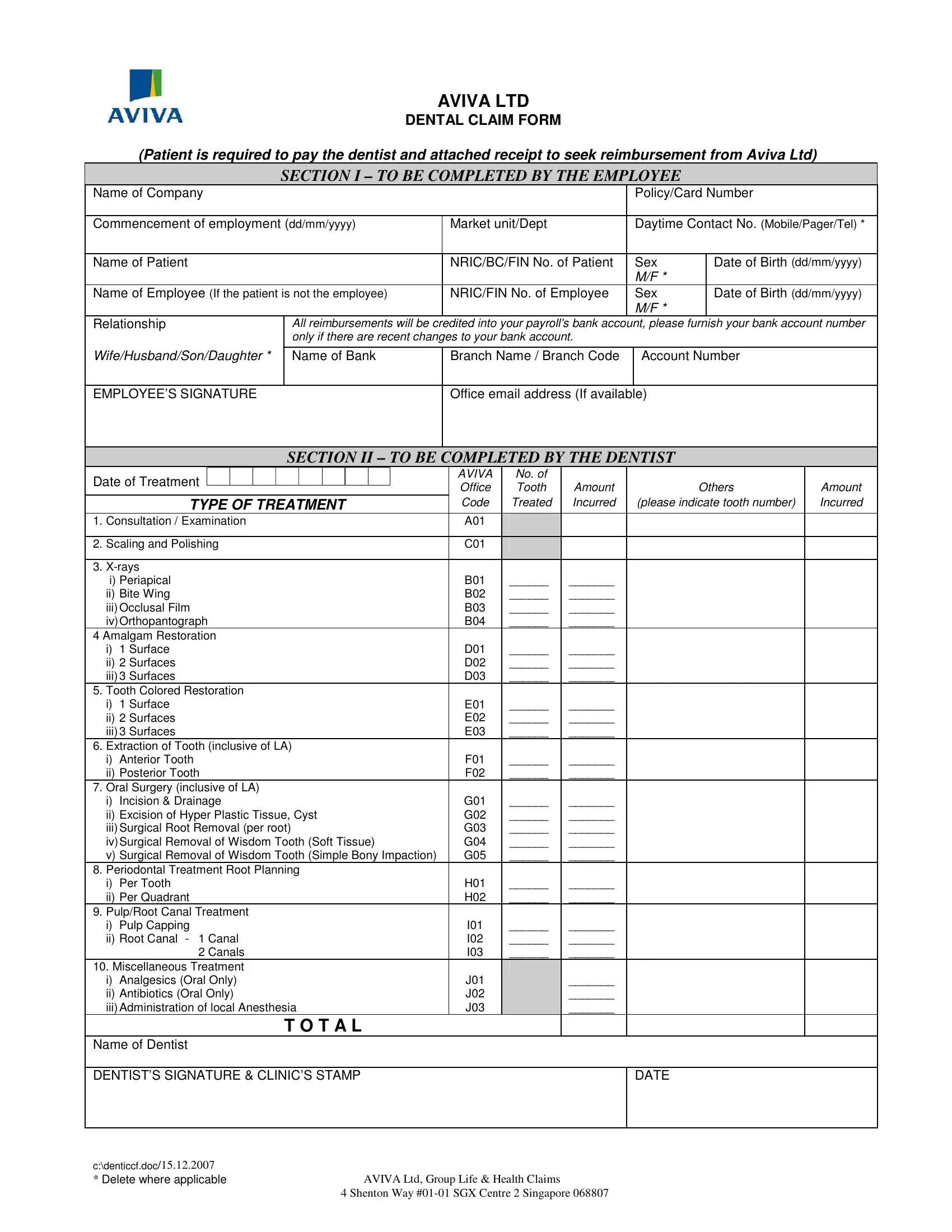
Navigating through the process of dental claims can seem daunting, yet with Aviva Ltd's structured and comprehensive Dental Claim Form, the process is streamlined for both the employee and the dentist involved. Designed with clarity in mind, this form is divided into two major sections: the first to be completed by the employee and the second by the dentist providing the treatment. Employees are obligated to initially cover the dental expenses and then attach the receipt to this form as a part of their reimbursement request from Aviva Ltd. Key personal and employment details including the policy or card number, and relationship to the patient if the claimant is not the patient themselves, are required in Section I. Additionally, for ease of transaction, employees are advised to update their bank account details if there have been any changes, facilitating direct credit reimbursements. Section II caters to the dental professionals, demanding specific information about the treatment provided, including the date, type of treatment dispensed, and costs incurred. The form also meticulously outlines different types of dental treatments and codes for easy identification and billing purposes. A signature from both the employee and the dentist at the end certifies the information provided, ensuring a smooth claim process. Lastly, a note underscores the importance of submitting the completed claim form alongside the treatment receipt to Aviva Ltd for processing, highlighting the company's commitment to expedite the reimbursement directly to the employee’s bank account, accompanied by a payment advice for complete transparency.
| Question | Answer |
|---|---|
| Form Name | AVIVA LTD Dental Claim Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 100 |
| Avg. time to fill out | 20 min 34 sec |
| Other names | aviva claim form pdf, aviva defer claim form, singapore aviva form online, aviva claim form |
AVIVA LTD
DENTAL CLAIM FORM
(Patient is required to pay the dentist and attached receipt to seek reimbursement from Aviva Ltd)
SECTION I – TO BE COMPLETED BY THE EMPLOYEE
Name of Company |
|
|
|
Policy/Card Number |
|
|
|
|
|
|
|
Commencement of employment (dd/mm/yyyy) |
Market unit/Dept |
|
Daytime Contact No. (Mobile/Pager/Tel) * |
||
|
|
|
|
|
|
Name of Patient |
|
NRIC/BC/FIN No. of Patient |
|
Sex |
Date of Birth (dd/mm/yyyy) |
|
|
|
|
M/F * |
|
Name of Employee (If the patient is not the employee) |
NRIC/FIN No. of Employee |
|
Sex |
Date of Birth (dd/mm/yyyy) |
|
|
|
|
|
M/F * |
|
Relationship |
All reimbursements will be credited into your payroll’s bank account, please furnish your bank account number |
||||
|
only if there are recent changes to your bank account. |
|
|
|
|
|
|
|
|
|
|
Wife/Husband/Son/Daughter * |
Name of Bank |
Branch Name / Branch Code |
|
Account Number |
|
|
|
|
|
|
|
EMPLOYEE’S SIGNATURE |
|
Office email address (If available) |
|
||
|
|
|
|
|
|
SECTION II – TO BE COMPLETED BY THE DENTIST
Date of Treatment |
|
|
|
|
|
|
|
|
|
|
AVIVA |
|
No. of |
|
|
|
|
|
|
|
|
|
|
|
|
|
Office |
|
Tooth |
Amount |
Others |
Amount |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
TYPE OF TREATMENT |
|
|
|
Code |
|
Treated |
Incurred |
(please indicate tooth number) |
Incurred |
|||||||
1. Consultation / Examination |
|
|
|
A01 |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
2. Scaling and Polishing |
|
|
|
C01 |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
3. |
|
|
|
|
|
|
|
|
|
|||||||
i) Periapical |
|
|
|
B01 |
|
______ |
_______ |
|
|
|||||||
ii) Bite Wing |
|
|
|
B02 |
|
______ |
_______ |
|
|
|||||||
iii) Occlusal Film |
|
|
|
B03 |
|
______ |
_______ |
|
|
|||||||
iv) Orthopantograph |
|
|
|
B04 |
|
______ |
_______ |
|
|
|||||||
4 Amalgam Restoration |
|
|
|
|
|
|
|
|
|
|||||||
i) 1 Surface |
|
|
|
D01 |
|
______ |
_______ |
|
|
|||||||
ii) 2 Surfaces |
|
|
|
D02 |
|
______ |
_______ |
|
|
|||||||
iii) 3 Surfaces |
|
|
|
D03 |
|
______ |
_______ |
|
|
|||||||
5. Tooth Colored Restoration |
|
|
|
|
|
|
|
|
|
|||||||
i) 1 Surface |
|
|
|
E01 |
|
______ |
_______ |
|
|
|||||||
ii) 2 Surfaces |
|
|
|
E02 |
|
______ |
_______ |
|
|
|||||||
iii) 3 Surfaces |
|
|
|
E03 |
|
______ |
_______ |
|
|
|||||||
6. Extraction of Tooth (inclusive of LA) |
|
|
|
|
|
|
|
|
|
|||||||
i) Anterior Tooth |
|
|
|
F01 |
|
______ |
_______ |
|
|
|||||||
ii) Posterior Tooth |
|
|
|
F02 |
|
______ |
_______ |
|
|
|||||||
7. Oral Surgery (inclusive of LA) |
|
|
|
|
|
|
|
|
|
|||||||
i) Incision & Drainage |
|
|
|
G01 |
|
______ |
_______ |
|
|
|||||||
ii) Excision of Hyper Plastic Tissue, Cyst |
|
|
|
G02 |
|
______ |
_______ |
|
|
|||||||
iii) Surgical Root Removal (per root) |
|
|
|
G03 |
|
______ |
_______ |
|
|
|||||||
iv) Surgical Removal of Wisdom Tooth (Soft Tissue) |
G04 |
|
______ |
_______ |
|
|
||||||||||
v) Surgical Removal of Wisdom Tooth (Simple Bony Impaction) |
G05 |
|
______ |
_______ |
|
|
||||||||||
8. Periodontal Treatment Root Planning |
|
|
|
|
|
|
|
|
|
|||||||
i) Per Tooth |
|
|
|
H01 |
|
______ |
_______ |
|
|
|||||||
ii) Per Quadrant |
|
|
|
H02 |
|
______ |
_______ |
|
|
|||||||
9. Pulp/Root Canal Treatment |
|
|
|
|
|
|
|
|
|
|||||||
i) Pulp Capping |
|
|
|
I01 |
|
______ |
_______ |
|
|
|||||||
ii) Root Canal - 1 Canal |
|
|
|
I02 |
|
______ |
_______ |
|
|
|||||||
2 Canals |
|
|
|
I03 |
|
______ |
_______ |
|
|
|||||||
10. Miscellaneous Treatment |
|
|
|
|
|
|
|
|
|
|||||||
i) Analgesics (Oral Only) |
|
|
|
J01 |
|
|
_______ |
|
|
|||||||
ii) Antibiotics (Oral Only) |
|
|
|
J02 |
|
|
_______ |
|
|
|||||||
iii) Administration of local Anesthesia |
|
|
|
J03 |
|
|
_______ |
|
|
|||||||
|
|
|
|
T O T A L |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||||||
Name of Dentist |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
DENTIST’S SIGNATURE & CLINIC’S STAMP |
|
|
|
|
|
|
|
DATE |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
c:\denticcf.doc/15.12.2007 |
|
|
|
|
|
|
|
|
|
|||||||
* Delete where applicable |
AVIVA Ltd, Group Life & Health Claims |
|
|
|
||||||||||||
4 Shenton Way
NOTE :-
1.Section I is to be completed by Employee.
2.Section II is to be completed by DENTIST.
3.Employee to pay the dentist after treatment and attached your receipt together with the completed claim form and submit to:-
Aviva Ltd
Group Life & Health Claims
4 Shenton Way
Singapore 068807
4.To expedite reimbursement, please provide your bank account for direct credit into your account. A payment advice will be sent upon credit to your bank account.
c:\denticcf.doc/15.12.2007 |
|
* Delete where applicable |
AVIVA Ltd, Group Life & Health Claims |
|
4 Shenton Way |