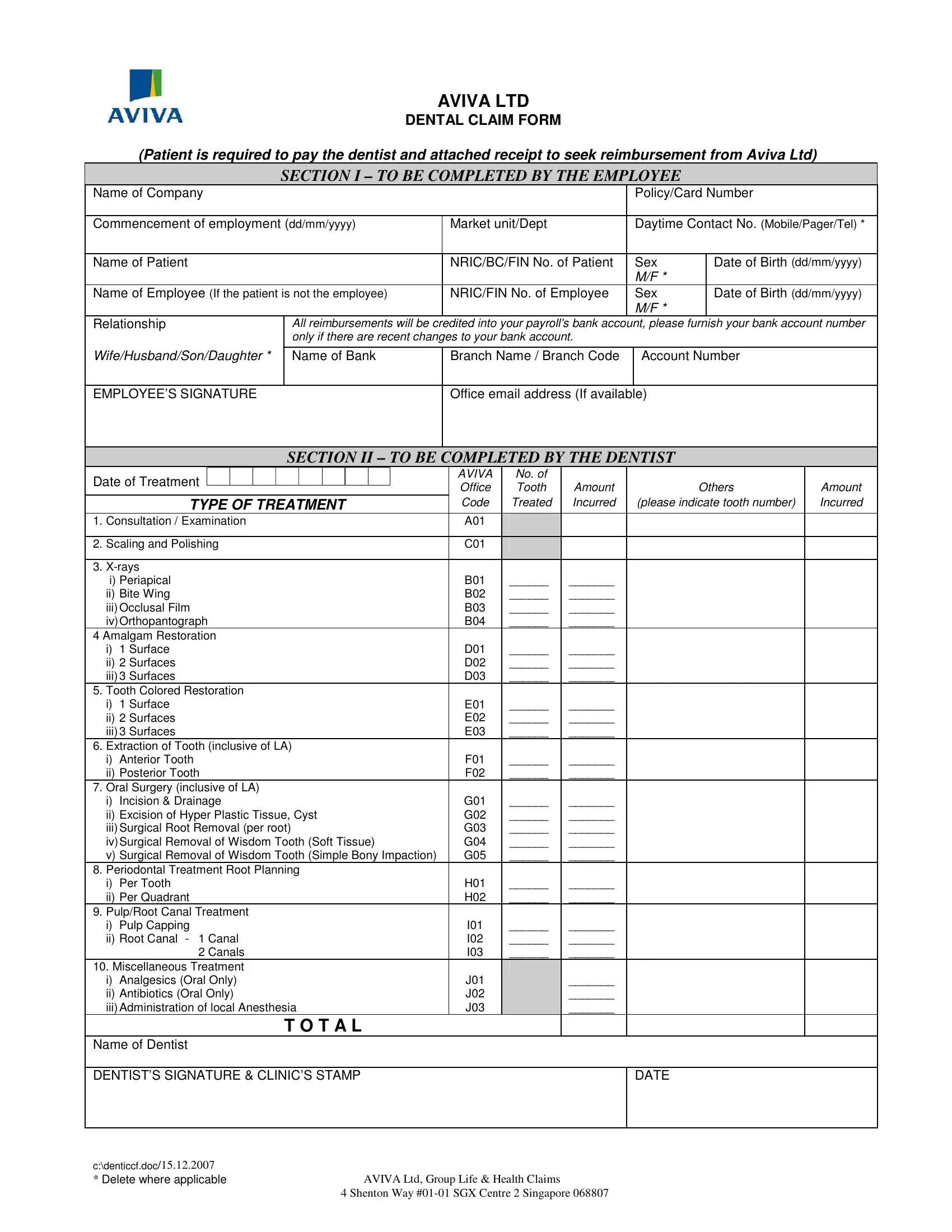
Aviva Ltd offers dental insurance to their policyholders. If you need to file a claim, here are the steps you need to take. First, download the dental claim form from the Aviva website. Next, fill out the form completely and accurately. Make sure to include your name, policy number, social security number, dentist's name and address, and the services provided. Finally, mail or fax the form to Aviva Ltd.
| Question | Answer |
|---|---|
| Form Name | Aviva Ltd Dental Claim Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | aviva dental insurance singapore, aviva claim form pdf, singapore aviva dental, aviva medical claim form |
AVIVA LTD
DENTAL CLAIM FORM
(Patient is required to pay the dentist and attached receipt to seek reimbursement from Aviva Ltd)
SECTION I – TO BE COMPLETED BY THE EMPLOYEE
Name of Company |
|
|
|
Policy/Card Number |
|
|
|
|
|
|
|
Commencement of employment (dd/mm/yyyy) |
Market unit/Dept |
|
Daytime Contact No. (Mobile/Pager/Tel) * |
||
|
|
|
|
|
|
Name of Patient |
|
NRIC/BC/FIN No. of Patient |
|
Sex |
Date of Birth (dd/mm/yyyy) |
|
|
|
|
M/F * |
|
Name of Employee (If the patient is not the employee) |
NRIC/FIN No. of Employee |
|
Sex |
Date of Birth (dd/mm/yyyy) |
|
|
|
|
|
M/F * |
|
Relationship |
All reimbursements will be credited into your payroll’s bank account, please furnish your bank account number |
||||
|
only if there are recent changes to your bank account. |
|
|
|
|
|
|
|
|
|
|
Wife/Husband/Son/Daughter * |
Name of Bank |
Branch Name / Branch Code |
|
Account Number |
|
|
|
|
|
|
|
EMPLOYEE’S SIGNATURE |
|
Office email address (If available) |
|
||
|
|
|
|
|
|
SECTION II – TO BE COMPLETED BY THE DENTIST
Date of Treatment |
|
|
|
|
|
|
|
|
|
|
AVIVA |
|
No. of |
|
|
|
|
|
|
|
|
|
|
|
|
|
Office |
|
Tooth |
Amount |
Others |
Amount |
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||||
TYPE OF TREATMENT |
|
|
|
Code |
|
Treated |
Incurred |
(please indicate tooth number) |
Incurred |
|||||||
1. Consultation / Examination |
|
|
|
A01 |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
2. Scaling and Polishing |
|
|
|
C01 |
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
3. |
|
|
|
|
|
|
|
|
|
|||||||
i) Periapical |
|
|
|
B01 |
|
______ |
_______ |
|
|
|||||||
ii) Bite Wing |
|
|
|
B02 |
|
______ |
_______ |
|
|
|||||||
iii) Occlusal Film |
|
|
|
B03 |
|
______ |
_______ |
|
|
|||||||
iv) Orthopantograph |
|
|
|
B04 |
|
______ |
_______ |
|
|
|||||||
4 Amalgam Restoration |
|
|
|
|
|
|
|
|
|
|||||||
i) 1 Surface |
|
|
|
D01 |
|
______ |
_______ |
|
|
|||||||
ii) 2 Surfaces |
|
|
|
D02 |
|
______ |
_______ |
|
|
|||||||
iii) 3 Surfaces |
|
|
|
D03 |
|
______ |
_______ |
|
|
|||||||
5. Tooth Colored Restoration |
|
|
|
|
|
|
|
|
|
|||||||
i) 1 Surface |
|
|
|
E01 |
|
______ |
_______ |
|
|
|||||||
ii) 2 Surfaces |
|
|
|
E02 |
|
______ |
_______ |
|
|
|||||||
iii) 3 Surfaces |
|
|
|
E03 |
|
______ |
_______ |
|
|
|||||||
6. Extraction of Tooth (inclusive of LA) |
|
|
|
|
|
|
|
|
|
|||||||
i) Anterior Tooth |
|
|
|
F01 |
|
______ |
_______ |
|
|
|||||||
ii) Posterior Tooth |
|
|
|
F02 |
|
______ |
_______ |
|
|
|||||||
7. Oral Surgery (inclusive of LA) |
|
|
|
|
|
|
|
|
|
|||||||
i) Incision & Drainage |
|
|
|
G01 |
|
______ |
_______ |
|
|
|||||||
ii) Excision of Hyper Plastic Tissue, Cyst |
|
|
|
G02 |
|
______ |
_______ |
|
|
|||||||
iii) Surgical Root Removal (per root) |
|
|
|
G03 |
|
______ |
_______ |
|
|
|||||||
iv) Surgical Removal of Wisdom Tooth (Soft Tissue) |
G04 |
|
______ |
_______ |
|
|
||||||||||
v) Surgical Removal of Wisdom Tooth (Simple Bony Impaction) |
G05 |
|
______ |
_______ |
|
|
||||||||||
8. Periodontal Treatment Root Planning |
|
|
|
|
|
|
|
|
|
|||||||
i) Per Tooth |
|
|
|
H01 |
|
______ |
_______ |
|
|
|||||||
ii) Per Quadrant |
|
|
|
H02 |
|
______ |
_______ |
|
|
|||||||
9. Pulp/Root Canal Treatment |
|
|
|
|
|
|
|
|
|
|||||||
i) Pulp Capping |
|
|
|
I01 |
|
______ |
_______ |
|
|
|||||||
ii) Root Canal - 1 Canal |
|
|
|
I02 |
|
______ |
_______ |
|
|
|||||||
2 Canals |
|
|
|
I03 |
|
______ |
_______ |
|
|
|||||||
10. Miscellaneous Treatment |
|
|
|
|
|
|
|
|
|
|||||||
i) Analgesics (Oral Only) |
|
|
|
J01 |
|
|
_______ |
|
|
|||||||
ii) Antibiotics (Oral Only) |
|
|
|
J02 |
|
|
_______ |
|
|
|||||||
iii) Administration of local Anesthesia |
|
|
|
J03 |
|
|
_______ |
|
|
|||||||
|
|
|
|
T O T A L |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|||||||
Name of Dentist |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
DENTIST’S SIGNATURE & CLINIC’S STAMP |
|
|
|
|
|
|
|
DATE |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|||||||
c:\denticcf.doc/15.12.2007 |
|
|
|
|
|
|
|
|
|
|||||||
* Delete where applicable |
AVIVA Ltd, Group Life & Health Claims |
|
|
|
||||||||||||
4 Shenton Way
NOTE :-
1.Section I is to be completed by Employee.
2.Section II is to be completed by DENTIST.
3.Employee to pay the dentist after treatment and attached your receipt together with the completed claim form and submit to:-
Aviva Ltd
Group Life & Health Claims
4 Shenton Way
Singapore 068807
4.To expedite reimbursement, please provide your bank account for direct credit into your account. A payment advice will be sent upon credit to your bank account.
c:\denticcf.doc/15.12.2007 |
|
* Delete where applicable |
AVIVA Ltd, Group Life & Health Claims |
|
4 Shenton Way |