As a dental provider, you may find that you need to complete a DC 37 form. This form is used to provide insurance and other benefits information for your patients. The form can be completed online or through the mail, and must be submitted every two years. Completing the form accurately is important, as it can help ensure that your patients receive the benefits they are entitled to. In this blog post, we will discuss how to fill out the DC 37 dental form correctly. We will also provide links to resources that can help you if you have any questions about completing the form. Thanks for reading!
| Question | Answer |
|---|---|
| Form Name | Dc 37 Dental Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | delta dental insurance dc37, 37 dental dc, dc37 delta dental list, ny form dc37 |
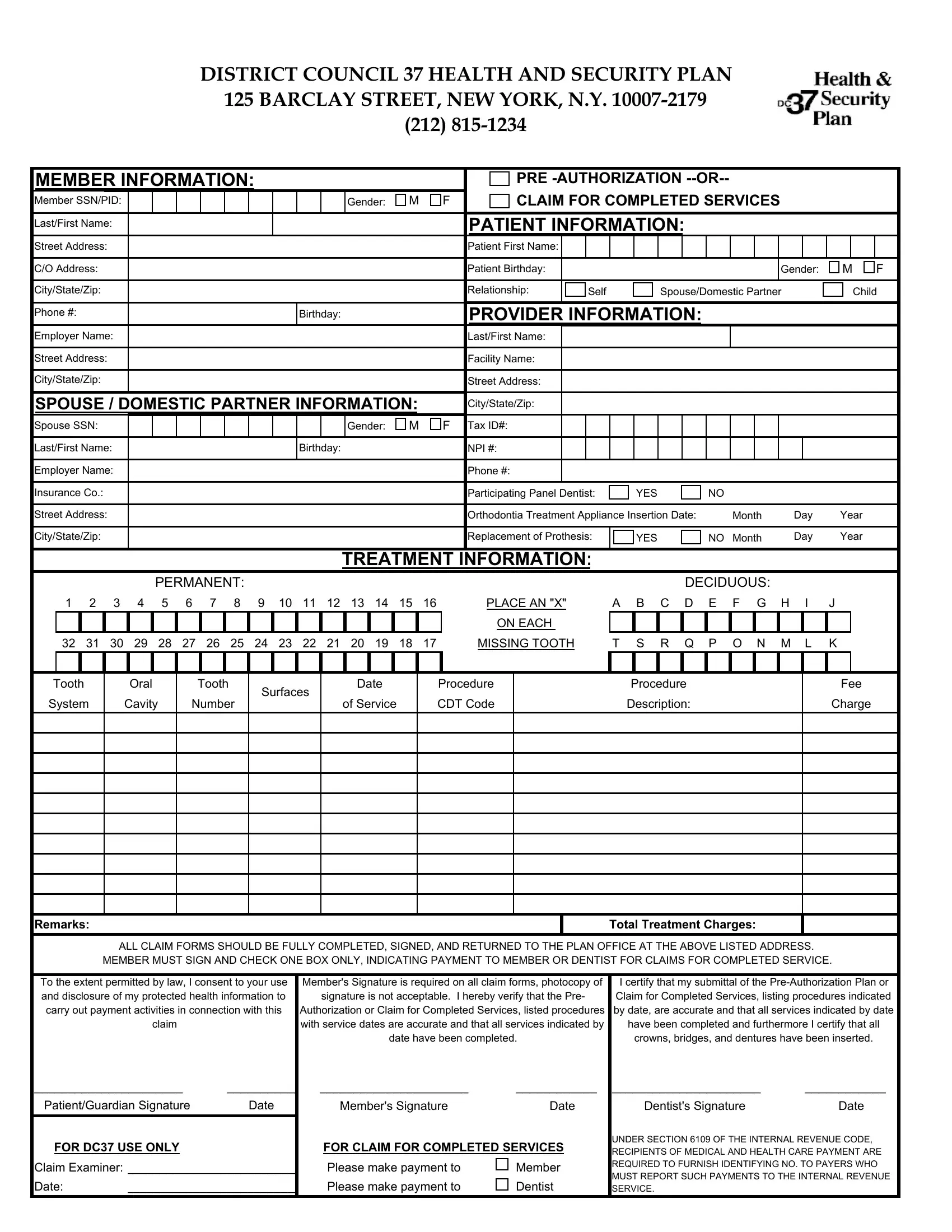
DISTRICT COUNCIL 37 HEALTH AND SECURITY PLAN 125 BARCLAY STREET, NEW YORK, N.Y.
|
MEMBER INFORMATION: |
|
|
|
|
|
|
|
|
|
|
|
PRE |
|
|
|
|
|
|
|
|
||||||||||||||||||||
Member SSN/PID: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gender: |
|
M |
|
F |
|
|
CLAIM FOR COMPLETED SERVICES |
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Last/First Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PATIENT INFORMATION: |
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Street Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient First Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
C/O Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Patient Birthday: |
|
|
|
|
|
|
|
|
|
Gender: |
M F |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
City/State/Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Relationship: |
|
Self |
|
|
Spouse/Domestic Partner |
|
|
|
Child |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone #: |
|
|
|
|
|
|
|
|
|
|
|
Birthday: |
|
|
|
|
|
PROVIDER INFORMATION: |
|
|
|
|
|
|
|
|
|
||||||||||||||
Employer Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Last/First Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Street Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Facility Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
City/State/Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Street Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
SPOUSE / DOMESTIC PARTNER INFORMATION: |
|
|
City/State/Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
Spouse SSN: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Gender: |
|
M |
|
F |
Tax ID#: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Last/First Name: |
|
|
|
|
|
|
|
|
|
|
|
Birthday: |
|
|
|
|
NPI #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Employer Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Phone #: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Insurance Co.: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Participating Panel Dentist: |
|
YES |
NO |
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
Street Address: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Orthodontia Treatment Appliance Insertion Date: |
|
Month |
Day |
Year |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
City/State/Zip: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Replacement of Prothesis: |
|
YES |
NO |
Month |
Day |
Year |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TREATMENT INFORMATION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
PERMANENT: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DECIDUOUS: |
|
|
|
|
|
||||||||
1 2 3 |
4 5 |
|
6 |
7 |
8 |
9 |
|
10 |
11 12 13 14 |
15 |
16 |
|
|
PLACE AN "X" |
|
A B C D |
E |
F G H |
|
I |
J |
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ON EACH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
32 31 30 29 28 27 |
26 |
25 |
24 |
|
23 |
22 21 20 19 18 17 |
|
|
MISSING TOOTH |
|
T S R Q P O N M L |
K |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Tooth |
|
|
Oral |
|
|
Tooth |
|
Surfaces |
|
Date |
|
|
Procedure |
|
|
Procedure |
|
|
|
|
|
|
Fee |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
System |
|
Cavity |
|
Number |
|
|
|
|
|
of Service |
CDT Code |
|
|
Description: |
|
|
|
|
|
|
Charge |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Remarks: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Total Treatment Charges: |
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
|
|
|
|
ALL CLAIM FORMS SHOULD BE FULLY COMPLETED, SIGNED, AND RETURNED TO THE PLAN OFFICE AT THE ABOVE LISTED ADDRESS. |
|
|
|
||||||||||||||||||||||||||||||||||
|
|
|
|
MEMBER MUST SIGN AND CHECK ONE BOX ONLY, INDICATING PAYMENT TO MEMBER OR DENTIST FOR CLAIMS FOR COMPLETED SERVICE. |
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
To the extent permitted by law, I consent to your use |
Member's Signature is required on all claim forms, photocopy of |
I certify that my submittal of the |
||||||||||||||||||||||||||||||||||||||
|
and disclosure of my protected health information to |
|
signature is not acceptable. I hereby verify that the Pre- |
|
Claim for Completed Services, listing procedures indicated |
||||||||||||||||||||||||||||||||||||
|
carry out payment activities in connection with this |
Authorization or Claim for Completed Services, listed procedures |
by date, are accurate and that all services indicated by date |
||||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
claim |
|
|
|
|
|
|
|
with service dates are accurate and that all services indicated by |
have been completed and furthermore I certify that all |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
date have been completed. |
|
|
crowns, bridges, and dentures have been inserted. |
||||||||||||||||||
______________________ |
|
|
__________ |
______________________ |
____________ |
______________________ |
|
____________ |
|||||||||||||||||||||||||||||||||
|
Patient/Guardian Signature |
|
|
Date |
|
|
Member's Signature |
|
|
Date |
|
|
Dentist's Signature |
|
|
Date |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FOR CLAIM FOR COMPLETED SERVICES |
|
UNDER SECTION 6109 OF THE INTERNAL REVENUE CODE, |
||||||||||||||||||||||
|
FOR DC37 USE ONLY |
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
RECIPIENTS OF MEDICAL AND HEALTH CARE PAYMENT ARE |
|||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Claim Examiner: _________________________ |
|
Please make payment to |
|
|
Member |
|
REQUIRED TO FURNISH IDENTIFYING NO. TO PAYERS WHO |
||||||||||||||||||||||||||||||||||
|
|
|
|
MUST REPORT SUCH PAYMENTS TO THE INTERNAL REVENUE |
|||||||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Date: |
_________________________ |
|
Please make payment to |
|
|
Dentist |
|
SERVICE. |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||