This form is used by AvMed members and their prescribing physicians to request access to medications outside the standard formulary. Two broad categories are covered: commercially available drugs that need a plan exception, and specialty or biologic medications administered in a physician's office or clinic. Knowing the scope, timelines, and documentation requirements helps you submit a complete request the first time.
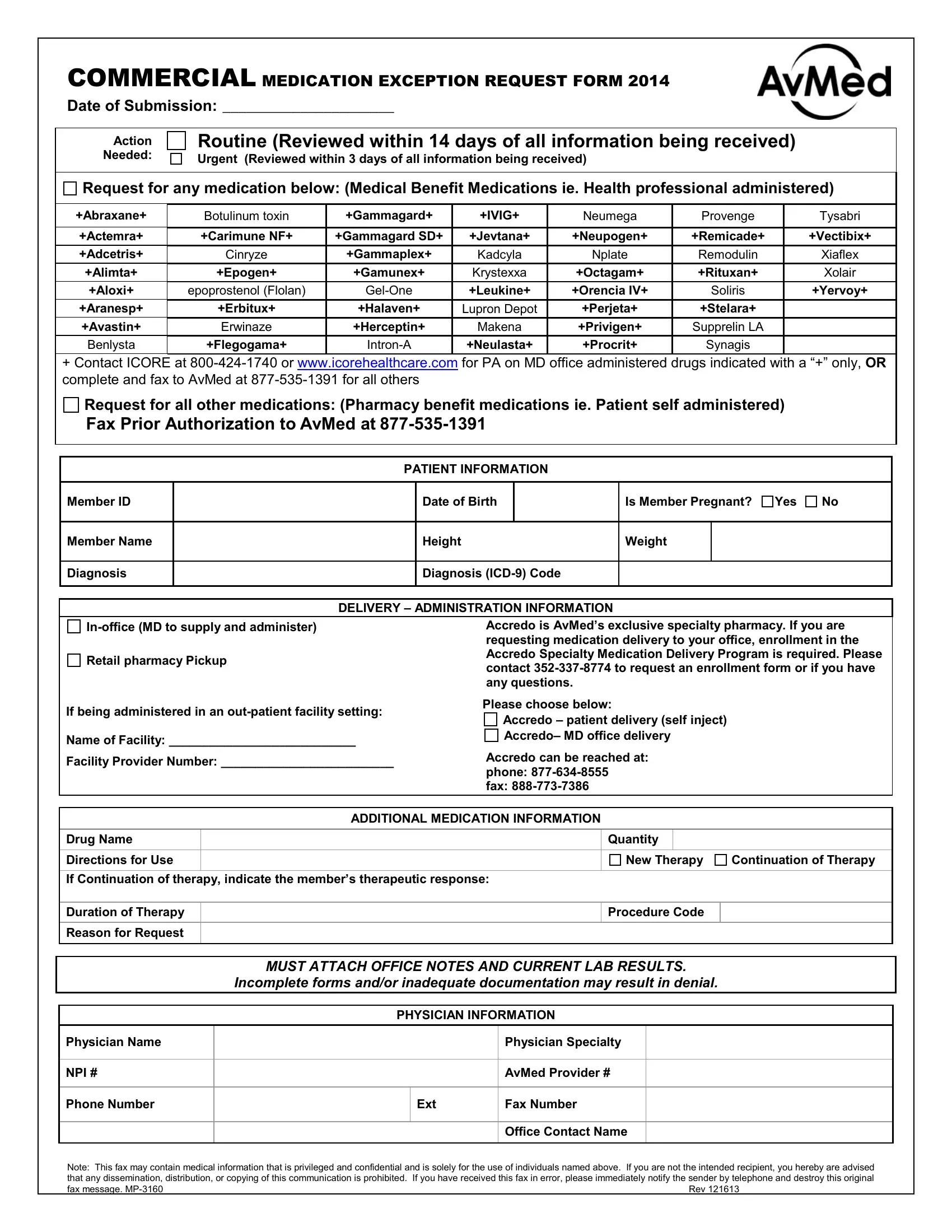
The form applies to a wide range of specialty and clinically administered drugs. Examples of covered medications include:
Any medication requiring prior authorization due to formulary status, administration method, or clinical complexity can be submitted through this process. Contact your physician's office if you are unsure whether your medication qualifies.
AvMed reviews requests on two tracks based on clinical urgency:
Discuss the appropriate track with your prescribing physician before marking the form. Incorrectly flagging a routine request as urgent may trigger an additional verification step and slow the review process.
Incomplete submissions are the leading cause of delays and denials. Prepare all of the following before submitting:
Lab results must reflect the patient's current clinical status. Older results from prior treatment periods may need to be supplemented with a physician note. Missing documentation restarts the review clock.
The form asks you to identify one of two administration pathways. Each follows a different approval and billing route:
Selecting the wrong delivery setting requires resubmission and resets the review timeline. Confirm the correct pathway with your physician before completing this section.
Once received, AvMed sends a confirmation to the prescribing physician's office and, where applicable, to the specialty pharmacy. The review team may request additional information during the evaluation period. Keep a copy of all submitted documents for your records. If no decision arrives within the applicable timeline, contact AvMed provider services to check on your request status.
| Question | Answer |
|---|---|
| Form Name | Avmed Request Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | INR, avmed report form, medco, pa |