
Y-Yes can be filled in easily. Just open FormsPal PDF tool to complete the task promptly. To maintain our tool on the cutting edge of practicality, we work to put into action user-oriented capabilities and improvements regularly. We are always pleased to get feedback - join us in revolutionizing PDF editing. Starting is easy! All you have to do is stick to the next easy steps directly below:
Step 1: Click the "Get Form" button in the top area of this webpage to access our editor.
Step 2: The tool will let you work with PDF files in a range of ways. Enhance it by including customized text, adjust what is already in the file, and add a signature - all close at hand!
As for the blanks of this specific form, this is what you should do:
1. Whenever filling out the Y-Yes, be certain to complete all of the needed blank fields within the associated section. It will help to speed up the process, making it possible for your information to be handled promptly and properly.
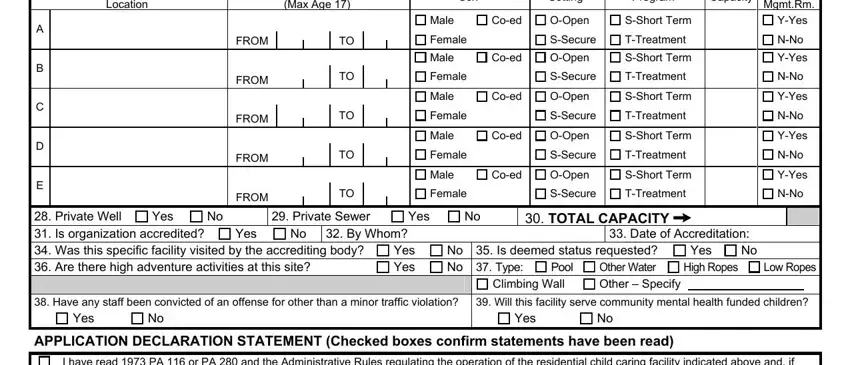
2. After filling in the last section, go to the next step and fill out the essential particulars in all these blank fields - Location, FROM, FROM, FROM, FROM, FROM, Age Range Max Age , Yes, Private Well Is organization, Private Sewer, Yes, By Whom, Sex, Setting, and Program.
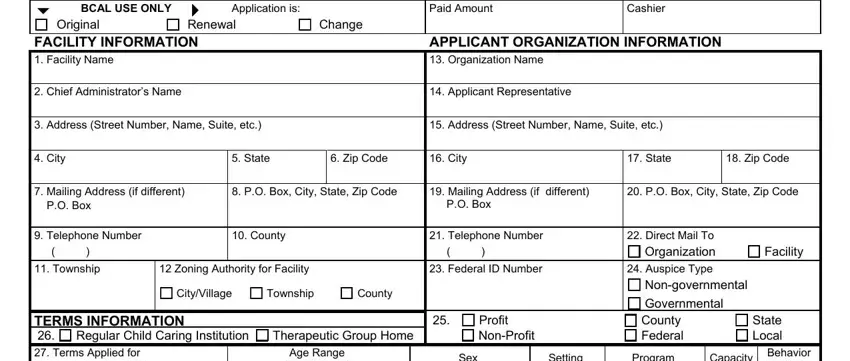
3. Completing I have read PA or PA and the, In order to permit a proper, I certify that the employees of, I hereby certify that any, Authorized Signature, Address Street Number and Name, Title, City, Date, State, Zip Code, BCAL Rev Previous editions, DISTRIBUTION When completed return, and Make a copy for your records is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
It is possible to make errors while completing the Date, so make sure to reread it before you'll send it in.
Step 3: Proofread everything you have typed into the blank fields and hit the "Done" button. Join us now and instantly gain access to Y-Yes, all set for downloading. All alterations made by you are preserved , allowing you to edit the file at a later point if necessary. FormsPal is dedicated to the confidentiality of our users; we always make sure that all personal data going through our system stays secure.