
You may prepare OREGON instantly using our PDF editor online. Our expert team is constantly working to develop the editor and make it much better for users with its handy features. Enjoy an ever-evolving experience now! This is what you'd need to do to start:
Step 1: Just click the "Get Form Button" at the top of this page to see our form editor. Here you will find all that is required to fill out your document.
Step 2: When you start the editor, you'll notice the document made ready to be filled in. In addition to filling in different blanks, you might also perform many other things with the file, such as writing any words, modifying the initial text, inserting images, placing your signature to the PDF, and much more.
When it comes to fields of this precise PDF, this is what you need to know:
1. To start with, while completing the OREGON, start in the form section that features the next blank fields:
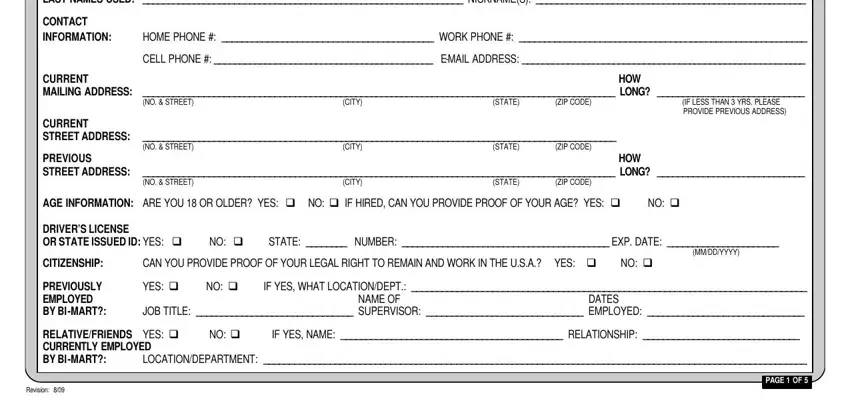
2. Once your current task is complete, take the next step – fill out all of these fields - FULL NAME ALL OTHER LAST NAMES, HOME PHONE WORK PHONE , CELL PHONE EMAIL ADDRESS , CITY, NO STREET, CITY, STATE, HOW, NO STREET, NO STREET, ZIP CODE, IF LESS THAN YRS PLEASE PROVIDE, CURRENT MAILING ADDRESS LONG , YES q NO q IF YES WHAT, and CAN YOU PROVIDE PROOF OF YOUR with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. This 3rd segment is considered rather easy, SCHOOLS ATTENDED, LAST JR HIGHMIDDLE SCHOOL, City State, LAST HIGH SCHOOL, City State, COLLEGEUNIVERSITY OR, NAME, City State, NAME, City State, CIRCLE HIGHEST, GRADE COMPLETED, WHAT NAMES ARE RECORDS UNDER, DIPLOMA OR GED, and YES cid - these form fields will have to be completed here.
4. Filling in DATE EMPLOYED, Month Year, MO YR MO YR FROM TO, TYPE OF BUSINESS, COMPANYORGANIZATION Complete Name , JOB TITLEDUTIES PERFORMED, AT START OF EMPLOYMENT, JOB TITLEDUTIES PERFORMED, AT END OF EMPLOYMENT, Name Street address City State, HOW WAS POSITION, OBTAINED, AVG HRS WORKED PER WEEK, SALARY, and START is crucial in this fourth form section - be certain to don't hurry and be mindful with each and every empty field!
It is easy to make a mistake while filling in your OBTAINED, hence be sure to reread it prior to deciding to finalize the form.
5. Because you approach the finalization of the document, there are just a few extra requirements that should be met. Notably, TYPE OF BUSINESS, Name Street address City State, HOW WAS POSITION, OBTAINED, AVG HRS WORKED PER WEEK, SALARY, START, UPON, LEAVING, NUMBER OF PEOPLE YOU SUPERVISED, REASON FOR LEAVING OR LOOKING, TO LEAVE BE SPECIFIC, IMMEDIATE SUPERVISOR, NAME TITLE PHONE MAY WE, and PAGE OF must be filled in.
Step 3: Prior to finishing your form, double-check that form fields have been filled in the right way. As soon as you’re satisfied with it, press “Done." After starting afree trial account with us, it will be possible to download OREGON or send it via email right away. The file will also be accessible from your personal cabinet with your changes. FormsPal ensures your information privacy by using a protected method that in no way saves or shares any personal information involved. You can relax knowing your paperwork are kept confidential every time you work with our editor!