
Using PDF files online is always super easy using our PDF editor. You can fill in cdcr acp application here painlessly. We are devoted to providing you the absolute best experience with our tool by continuously presenting new functions and enhancements. With all of these updates, working with our editor becomes easier than ever! This is what you will have to do to get going:
Step 1: Simply hit the "Get Form Button" in the top section of this webpage to start up our pdf editor. There you will find all that is necessary to work with your document.
Step 2: With our handy PDF editing tool, it is easy to do more than merely fill out forms. Edit away and make your forms look great with custom textual content added in, or optimize the file's original content to perfection - all comes with the capability to add any graphics and sign the file off.
As for the blanks of this particular form, this is what you should consider:
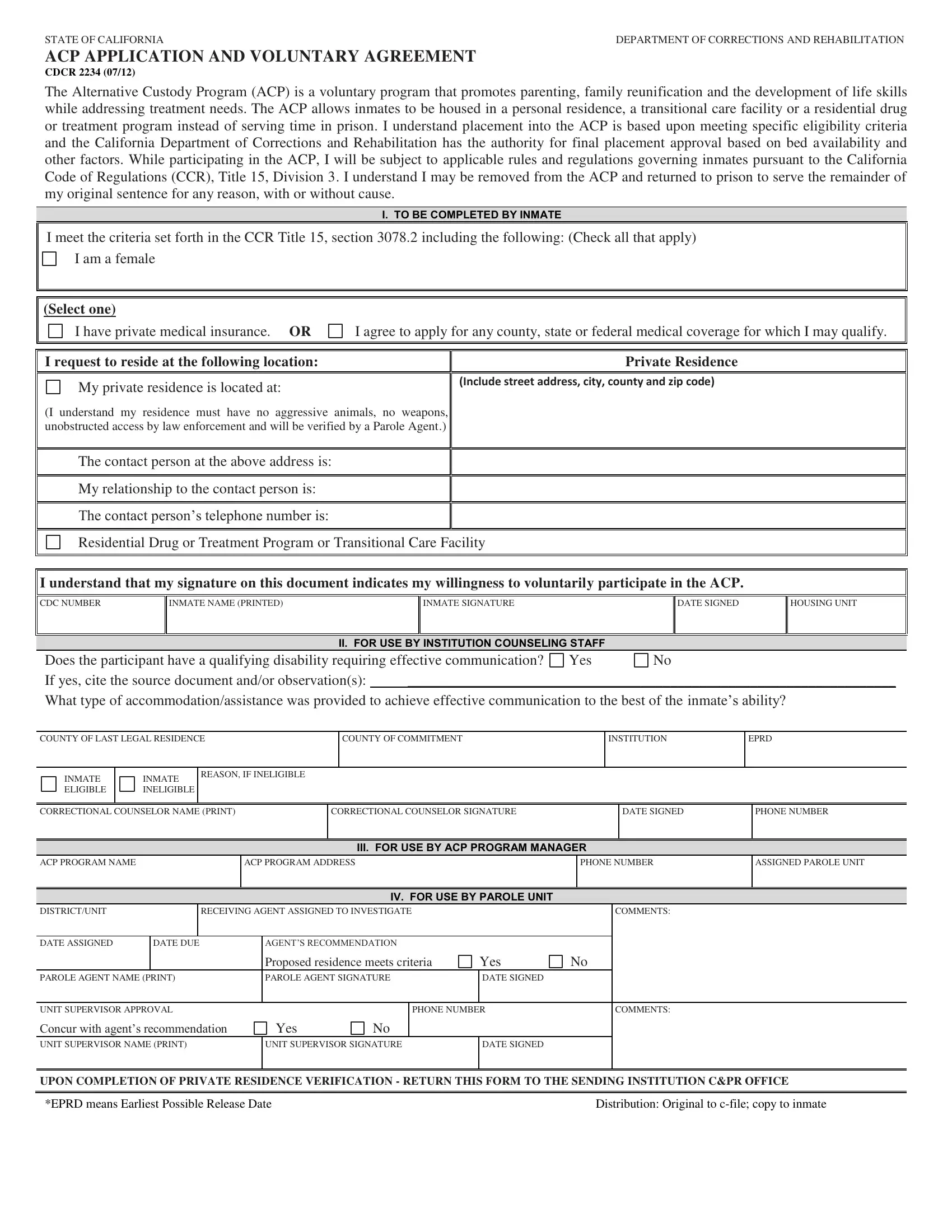
1. Complete your cdcr acp application with a selection of major blank fields. Gather all the required information and be sure absolutely nothing is overlooked!
2. Immediately after this part is filled out, proceed to type in the suitable information in all these - INMATE ELIGIBLE, INMATE INELIGIBLE, REASON IF INELIGIBLE, CORRECTIONAL COUNSELOR NAME PRINT, CORRECTIONAL COUNSELOR SIGNATURE, DATE SIGNED, PHONE NUMBER, III FOR USE BY ACP PROGRAM MANAGER, ACP PROGRAM NAME, ACP PROGRAM ADDRESS, PHONE NUMBER, ASSIGNED PAROLE UNIT, DISTRICTUNIT, RECEIVING AGENT ASSIGNED TO, and COMMENTS.
It is easy to make a mistake when filling out the DATE SIGNED, and so make sure you go through it again before you decide to submit it.
Step 3: Prior to submitting your document, check that all blank fields were filled out right. The moment you are satisfied with it, click on “Done." After setting up afree trial account here, you will be able to download cdcr acp application or send it via email at once. The PDF form will also be available through your personal account menu with all of your changes. FormsPal provides safe document editing with no personal data recording or distributing. Rest assured that your details are in good hands here!