
Any time you wish to fill out california dwc 906, there's no need to download and install any sort of software - simply try using our online tool. In order to make our editor better and simpler to utilize, we constantly come up with new features, with our users' feedback in mind. It merely requires a few easy steps:
Step 1: Access the PDF doc in our tool by clicking the "Get Form Button" at the top of this page.
Step 2: This tool will allow you to modify nearly all PDF forms in various ways. Change it with customized text, adjust original content, and put in a signature - all within several clicks!
This document will require specific information; in order to guarantee consistency, please bear in mind the following steps:
1. Whenever submitting the california dwc 906, be certain to complete all needed blank fields in the associated form section. This will help to expedite the process, making it possible for your details to be handled efficiently and appropriately.
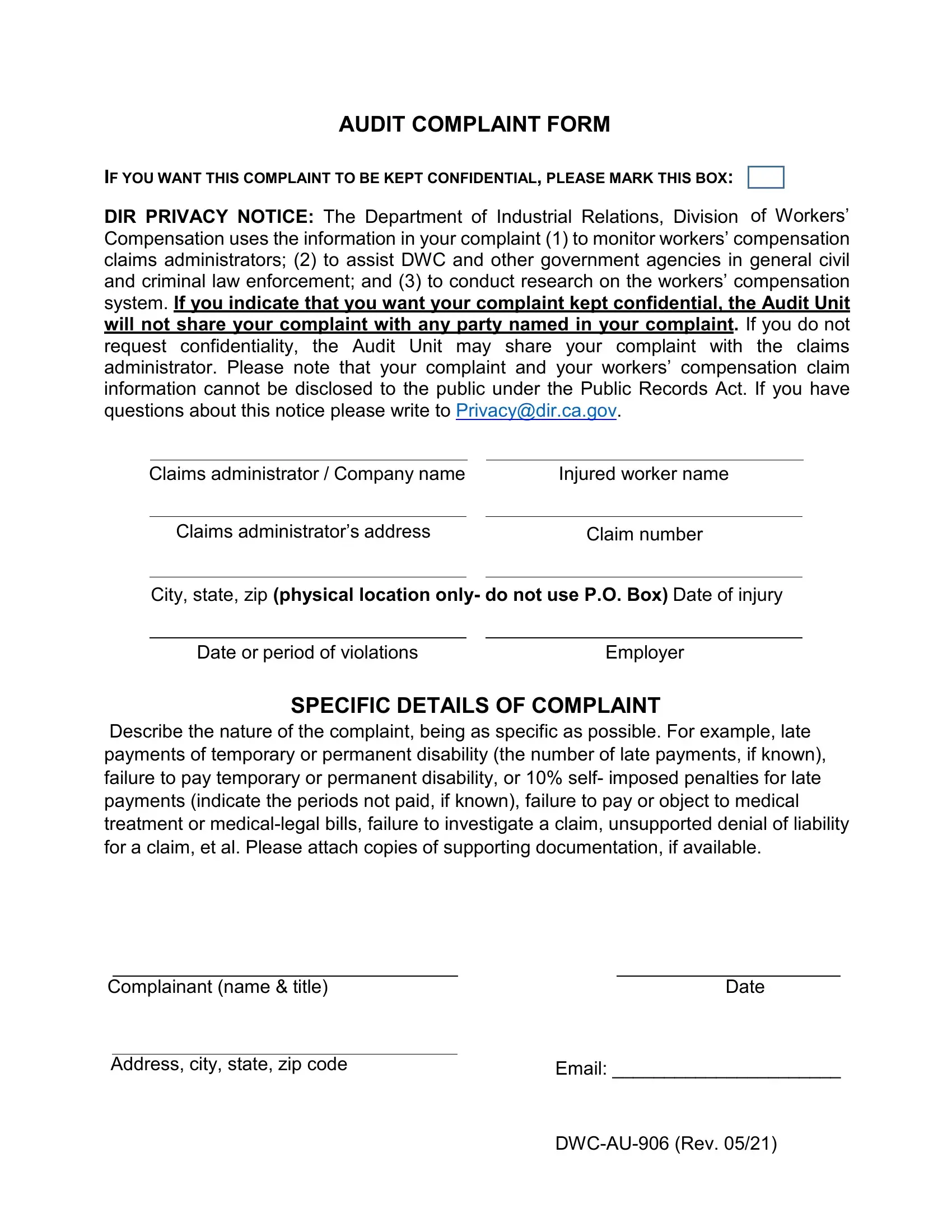
2. Just after finishing the last step, go to the next step and complete the necessary details in all these blank fields - Describe the nature of the, Complainant name title, Date, Address city state zip code, Email , and DWCAU Rev .
It's easy to get it wrong when completing your Date, thus ensure that you look again before you send it in.
Step 3: Look through all the information you've inserted in the form fields and hit the "Done" button. Right after getting afree trial account here, it will be possible to download california dwc 906 or send it through email directly. The document will also be available from your personal cabinet with all your edits. At FormsPal, we endeavor to be sure that all of your information is kept private.