In the joyous and often overwhelming journey of welcoming a new member into the family, parents in California are introduced to the "Certificate of Live Birth Worksheet," a critical document that lays the initial groundwork for their child’s legal and social identity. Designed with both simplicity and comprehensiveness in mind, this form requests essential details that will adorn the official birth certificate, a document of paramount importance that proves a child’s age, parentage, and citizenship. This document bears the significant responsibility of safeguarding the child's privacy and is protected under state laws to prevent the unauthorized release of identifying information. While primarily serving legal purposes, the data collected also contributes to health and medical research aimed at improving the welfare of mothers and newborns. Interestingly, the form touches on various aspects of the newborn's and parents’ life, ranging from the basic—such as the baby’s name, parents' names, and residential information—to specifics like racial background, education levels, and even smoking habits during pregnancy. Particular attention is paid to the type of birth, including the facility and the exact location, thereby ensuring that every child’s entry into the world is documented with precision. The worksheet also navigates through more sensitive territory, with options to apply for a Social Security Number for the newborn and questions about adoption. It’s a comprehensive tool designed not just for bureaucratic purposes but as a means to better understand and serve the population through detailed record-keeping.
| Question | Answer |
|---|---|
| Form Name | California Birth Certificate Editable Free Form |
| Form Length | 12 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min |
| Other names |
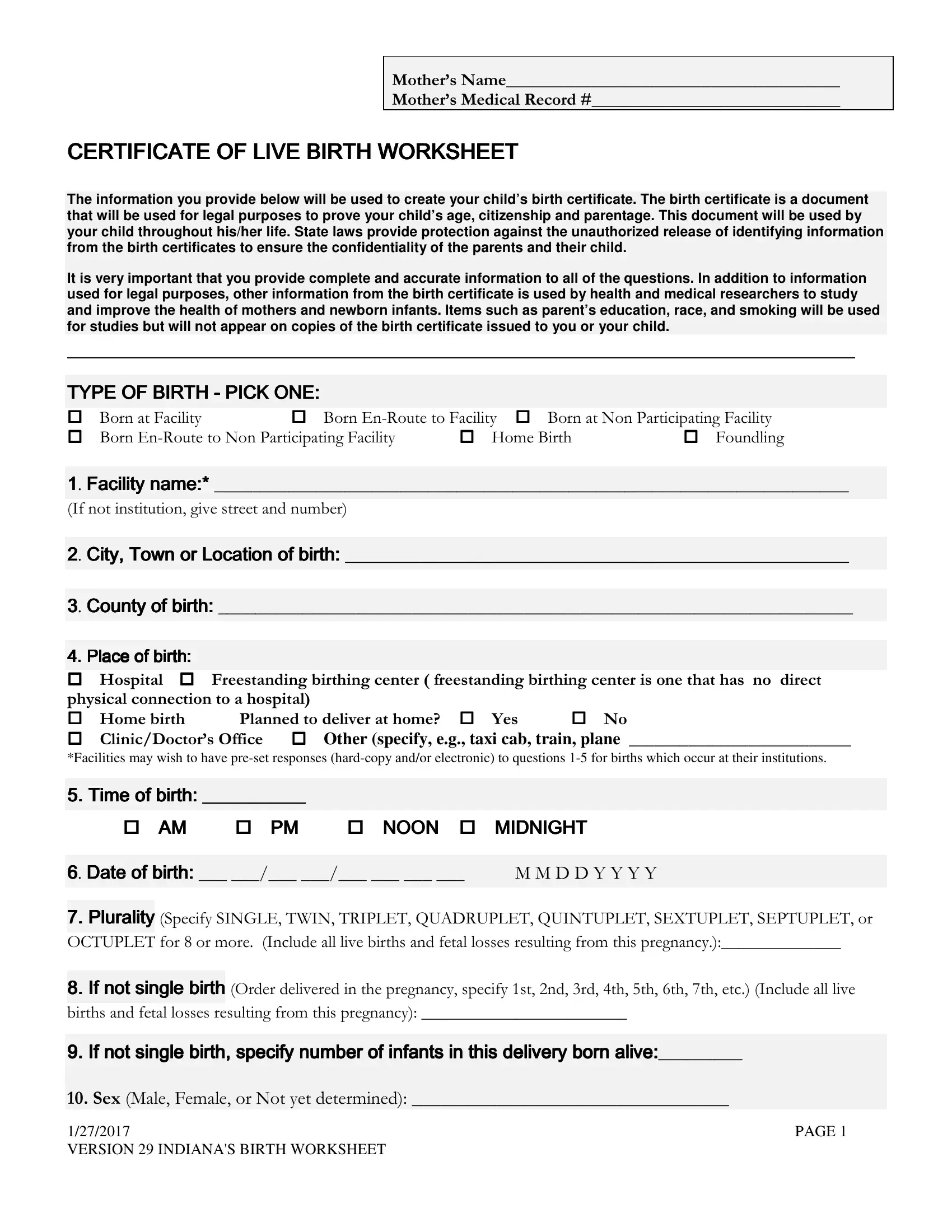
CERTIFICATE OF LIVE BIRTH WORKSHEET
The information you provide below will be used to create your child’s birth certificate. The birth certificate is a document that will be used for legal purposes to prove your child’s age, citizenship and parentage. This document will be used by your child throughout his/her life. State laws provide protection against the unauthorized release of identifying information from the birth certificates to ensure the confidentiality of the parents and their child.
It is very important that you provide complete and accurate information to all of the questions. In addition to information used for legal purposes, other information from the birth certificate is used by health and medical researchers to study and improve the health of mothers and newborn infants. Items such as parent’s education, race, and smoking will be used for studies but will not appear on copies of the birth certificate issued to you or your child.
TYPE OF BIRTH - PICK ONE:
|
|||||
|
|||||
1Facility name:*
!"#
2City, Town or Location of birth:
3County of birth:
4. Placeof birth:
|
|||
! |
|||
"#$% Other (specify, e.g., taxi cab, train, plane __________________________
*Facilities may wish to have
5 Time |
___________ |
|
|
|
|
|
|
AM |
PM |
NOON MIDNIGHT |
|
|
|
|
|
6Date of birth: $$ |
%%&&'''' |
||
|
|
|
|
7.Plurality (()* +, +*+
12+.*+3!"#4
8.If not single birth 1! 5 6 7 8 9 : ; #!
"#4
9. If not single birth, specify number of infants in this delivery born alive:
&'()*% #4
1/27/2017 |
PAGE 1 |
VERSION 29 INDIANA'S BIRTH WORKSHEET |
|
11. What will be your BABY’S legal name (as it should appear on the birth certificate)?
% |
* |
(<= # |
12. MOTHER: What is your current legal name?
|
+ |
||||||
|
|
|
|
|
|
|
13. MOTHER: Where do you usually
"4
(& ( /!
&/"
(4.(+ 2!# /0)."ountry
2 +> *424?4
14. Is this household inside city limits (inside the incorporated limits of the city, town or location
where you live)? ' &@A>
(B)<CD
15"4. MOTHER:What is your mailing address?
(& ( /!
&/"
(4.(+ 2!#
/0)."ountry
2 +> *424?4
6. |
What is your date of birth? (Example: |
||
|
|
|
|
$$ |
%%&&'''' |
1234 |
|
|
|
|
|
17. MOTHER: In what State, U.S. territory, or foreign country were you born? Please specify one
of the following:
(22 1.( .(E ) /(%
1
%534/,60()(6*67,6( /8",6,
/8"6,
09%8 |
||
|
|
|
18. MOTHER: What is your Social Security Number? |
||
|
|
|
|
______ ______ |
|
|
||
19. Do you want a Social Security Number issued for your baby? |
||
|
|
|
1/27/2017 |
PAGE 2 |
|
VERSION 29 INDIANA'S BIRTH WORKSHEET
!7,6 ",
(@signthI requestSocial.)thatSecuritythe SocialAdministrationSecurity Administratiwith the infonrmassigntionfroma Socialthis formSecuritywhichnumberis neededto thetochildassignnamednumberon this.(Eitherformandparent,authorizethethel galStateguardian,to providemay
&4$$ %%&&''''
20. Will infant be placed fo Adoption?
!
21.MOTHER: What is the highest level of schooling that you will have completed at the time of delivery? (Check the box that best describes your education. If you are cu rently enrolled, check
the box that indicates the previous grade or highest degree received).
3 |
F56 |
|||
)& |
(" |
|||
/// /(# |
@/ / (# |
|||
%@%/ %( % % %(, %/#
&& %& &&( &E% ** =
::(%5348,,,,,6,6; 6(
*,,5."1.8.";.(.,6,6; $).+6...(
0,%,4
0,/,4
Unemployed |
Unknown |
23. MOTHER: Are you Spanish/Hispanic/Latina? If not Spanish/Hispanic/Latina, check the “No” box. If Spanish/Hispanic/Latina, check the appropriate box.
($$*
' %< %</ 2 '
' 2"
' ($$*( (! & 2"#
#
24. MOTHER: What is your race? (Please check all that apply).
, |
A// |
|
|||||
//A!"## |
|||||||
|
|||||||
/ |
2 |
|
|||||
= |
G |
E |
|
||||
1/# |
|||||||
!> |
)2 |
( |
|||||
1# 1#
MOTHER: Additional Information To Be Filled In If A PATERNITY AFFIDAVIT IS TO BE FILED FOR THIS BIRTH If Not Filing Paternity Affidavit skip to question 30.
25.What is Your Phone Number? Required ________________________________________________
26.What is the name of your Employer (Company name)? Optional
|
|
1/27/2017 |
PAGE 3 |
VERSION 29 INDIANA'S BIRTH WORKSHEET |
|
27. What is your Employer's address? Optional
28. What is the name of your Medical Insurance Company? Optional
29. What is your Medical Insurance Policy number? Optional
30. MOTHER: Did you receive WIC (Women, Infants & Children) food for yourself because you were pregnant with this child?
! 0;6
31. MOTHER: What is your height? |
|
|
32. MOTHER: What was your
33. Mother’s weight at delivery "
34.CIGARETTE SMOKING BEFORE AND DURING PREGNANCY: How many cigarettes OR packs of cigarettes did you smoke on an average day during each of the following time periods?
If you NEVER smoked, enter zero for each time period.
+" |
#of cigarettes |
1# of packs |
|||
1 |
|||||
( |
1 |
||||
* |
1 |
||||
|
|
|
|
|
|
|
|
|
|
|
|
<=("0351/51+)5150) |
|
|
|||
!% |
|
|
|||
,> |
|
|
|
||
&! |
|
|
|
||
2% |
|
|
|
||
% "@
.A>
<>(Mother's name prior to her first marriage, (Maiden Name)
+ ),*
<?(%53@)),.13!%01/3$5%53153%!%0"/+$
BC7F
Yes |
|
|
|
BC73 |
|
||
|
|
|
|
|
|
|
|
<A(/.1 |
|
||
No |
' !" |
|
|
|
If Yes Date Affidavit was signed: ____ ____/____ ____/____ ____ ____ ____ |
||
|
|||
|
|
|
|
1/27/2017 |
|
|
PAGE 4 |
VERSION 29 INDIANA'S BIRTH WORKSHEET |
|
||
!"
If No please go to question 53
39. FATHER'S CURRENT LEGAL NAME
% |
* |
(<= # |
40. FATHER: What is the father's date of birth? (Example:
$$%%&&'''' 1234
41. FATHER: In what State, U.S. territory, or foreign country was he born? Please specify one of
the following:
(22 1.( .(E ) /(%
1
1534/60()(6*67,6( /8",6
/8"6
09%8
42.What is the father’s Social Security Number? If you are not married, or if a paternity acknowledgment has not been completed, leave this item blank.
43. What is
delivery? (Check the box that best describes his education. If he is currently enrolled, check the box that indicates the previous grade or highest degree received).
|
|
|
|
|
3 |
F56 |
|||
)& |
(" |
|||
/// /(# |
@/ / (# |
|||
%@%/ %( % % %(, %/#
&& %& &&( &E% ** =
BB(8@,,,,(6(*,
..,.(.,66;.);;.1.
(
0,%,4
0,/,4
Unemployed |
Unknown |
45. Is the father Spanish/Hispanic/Latino? If not Spanish/Hispanic/Latino, check the “No” box. If
Spanish/Hispanic/Latino, check all that apply.
($$*
1/27/2017 |
PAGE 5 |
VERSION 29 INDIANA'S BIRTH WORKSHEET |
|

' %< %</ 2 '
' 2"
' ($$*( (! & 2"#
#
46. What is the father’s race? Please check one or more races to indicate what he considers himself to be.
|
|
|
|
|
|
|
|
, |
A// |
|
|||||
//A!"# |
|||||||
|
|
||||||
/ |
2 |
|
|||||
= |
G |
E |
|
||||
1/# |
|||||||
!> |
)2 |
( |
|||||
1# |
|||||||
1# |
|||||||
|
|||||||
FATHER Additional Information To Be Filled In If A PATERNITY AFFIDAVIT IS TO BE FILED |
|||||||
|
|
||||||
FOR THIS BIRTH |
If Not Filing Paternity Affidavit skip to question 53 |
||||||
|
|
|
|
|
|
|
|
47.What is Your Phone Number? Information is required __________________________________
48.What is Your Current AddressNumber, Street, City, State and Zip Information is required
49.What is the name of your Employer (Company name)? Information is optional
50.What is your Employer's address? Information is optional
51. What is the name of your Medical Insurance Company? Information is optional
52. FATHER What is your Medical Insurance Policy Number Information is optional
=<($/$%533"3/C33151+"13
!3) |
% |
09%8 |
=B($">
<$>#
%%&&''''
==($!@#
%%&&'''' |
||
|
|
|
56. Source of |
|
|
|
|
|
1/27/2017 |
PAGE 6 |
|
VERSION 29 INDIANA'S BIRTH WORKSHEET |
|
|
=?(5,Other,2!Specify:
HIJ#4
=A($4%%&&''''
=D(,,6&!
5">A#4"I
|
|
|
|
|
|
|||
|
|
MD |
DO |
|
Clinic |
|
||
|
>'(,,6&! |
|||||||
|
5">A#4 |
|||||||
|
"I |
|||||||
|
|
|
|
|
|
|
|
|
|
>&($ |
$%%'''' |
||||||
>:(5,,
$>! !
"##
"I4 |
><($,&>> !"#4
$%%''''
>B(;2A#4
$E2,7,
&#
)&#
E3,..(
2#!""! #
&#
) #!""!
#&#%#>K
K> > #
>>KK%
#
!"L#!"7;>A
1! $>"#
6I>A
#
L/C
2 # /+#
E )+?+#
|
Fertili y enhancing drugs, artificial insemination, intrauterine ins mi ation ( Any |
|
2 # |
||
|
Assisted |
technology |
in vitro%!!!!!"<fertilization (IVF),reproductivegamete intrafallopiantechnology– transferAnyassisted(GIFT),reproductionZIFT) used to initate the(ART)"pregnancytechnical. procedures(e.g.
">#
' > |
||
|
|
Antiretrovirals administered during pregnancy or at delivery |
|
|
Group B Strep |
|
|
1/27/2017 |
PAGE 7 |
|
VERSION 29 INDIANA'S BIRTH WORKSHEET |
|
|
>=(/#,
>>#2A#4
)!
(!
2!#
E E!!#
2/ 2E!2!#
66. Was a Standard Licensed Diagnostic test for HIV performed for the Mother?
|
|
|
|
|
|
YES |
Yes give the date thespecimen was taken: |
|
(MMD YYYY) |
||
If Yes when was the test performed? |
During pregnancy |
|
|
||
|
|
|
|
Time of Delivery |
|
NO |
If No give reason (checkone below) |
|
|
||
|
Mother's Refusal |
HIV Status Know |
|
|
|
|
|
unknown) |
Insurance would not pay |
||
Other (specify): _______________________________________________________ |
|||||
Unknown (Reason why there was no est is |
|
|
|
||
>?(%,Unknown (Unknown%!!whether or not the test was$performed.)!
"$!#2A
#4
2!2"!<!!%&@
(A "!#
+L/>"<# <!L/!!<"<#
( |
|
||
|
|
|
>A(8,;, F!F
/!.04
>D(8))
!3)/!6;4$$!!!!
/!66 F$, |
F5$ |
%/;6
@, |
F)),96 |
%4
0;666,;6
0;60;666
70.Onset of Labor 2A#4
1/27/2017 |
PAGE 8 |
VERSION 29 INDIANA'S BIRTH WORKSHEET |
|
%"MN56( "A
">#56"""#
"O7#*"7#
"MN6I#*">6I
71. Characteristics of labor and delivery 2A#4
""P!"
"#
/"("!C>
!#
!<!< " ">
!!"!!<#
(#!"!" < !!<
!#
/"!"""!!
#!">"!
2"M7325II8#2
""!.>Q!
$" A/"!7325II8#
%$!"">
"P!>>#
">>>A4!
!!.!>Q <
! "
<>Q
1!!!!!! !
!#
"/"
!>">"#
/"
72.Method of delivery +">!>#
2/ 2
/,!>"R1">
!!# |
' |
||
|
|
|
,!>!<"RE!>
!!# |
' |
|||
|
|
|
|
|
2"2A#4 |
|
|
||
|
2!< 1/# 1## |
|||
|
" " A" "# |
|||
|
1/"!# |
|
||
|
|
|
|
|
&!2A#4 |
|
|||
|
E$(&!!"">> |
|||
!# |
|
|||
|
E$&!!""# |
|||
|
E$E&!!"!! |
|||
# |
|
|
||
|
2< "" |
|||
># |
|
|
||
>"R*">> >! |
||||
!# |
|
|
||
|
|
' |
|
|
|
|
|
|
|
1/27/2017 |
|
|
PAGE 9 |
|
VERSION 29 INDIANA'S BIRTH WORKSHEET |
|
|||
?<((<">"!# 2A#4
%>"A">"!#
+7<A !
"8"!><#
+>#
.(!>"
!#
/!/$!!#
.>!/"A!
>!<"#
?B(G64
21)4 %0$)#%0"3)4
?=(%>A#4
+"@" "<&"
"#
?>(1/!S!"#
(=I5I |
||||
9>4 |
|
|
||
(&'I5I Not Taken |
Unknown |
|
||
??16&"<">"# 2A#4
/!C>!!">"A
"">!"<<
#
/!C<!!"#" M:! C P!2/#
2./C!!
>"#
>"!!
"T"<
#
/"!">"/"
<#!!#
(K(K!! !!!"!(
!" <
<"<>2(
#
("TA# !T $$>C
!#&>!!"
>A "<!!(C !P"!<!>#
<! P<"!P!P
("! #
?A("6%>"
!# 2A#4
/""A/ ""/
>>#
%$("(P"
%%
>#"!>A#
1/27/2017 |
PAGE 10 |
VERSION 29 INDIANA'S BIRTH WORKSHEET |
|
"&"">
#
22>"4
!# !! P
!>>"#
2&>"
!#
1/"> ""
>""A+!"" ">#
/<&"!"A##
)/""> " "
!&""!
"#
*"<>#2"
<>!#
2*>>2%" "#
2!%"<
2"H>>2J"!#
&>(+65#
G2
G
Unknown |
|||
|
|
||
("> |
|||
A>""# |
|||
G2 |
|||
G |
|||
|
|||
!
! #
Microcephaly |
?D(86:B, 2AHJ>
>68! >
>#
' |
|
Unknown |
|||||||
|
|
|
|
|
|
|
|
||
4Unknown |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A'(/ !"" |
|||||||||
/>H'J"# |
|
||||||||
' |
|
A> |
|||||||
|
|
|
|
|
|
|
|
|
|
A&(/ |
|
|
|
|
|
||||
' |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
A:(G/,H |
|
|
|
|
|
||||
' |
|
Unknown |
|||||||
' &!4$$
83. Attendant’s name, title, and N.P.I
/@
Attendant’s title: |
&1 |
2%$2%2%>$2%># |
||
%& |
||||
1%>%>2%$2%# |
|
|||
1/27/2017 |
|
|
|
PAGE 11 |
VERSION 29 INDIANA'S BIRTH WORKSHEET |
|
|||
1#4
AB(/"1
'
|
Unknown |
|
/%6"7, |
||
|
|
A=("4
+!>"%" "" "#
%& |
&1 |
|
2%$2%2%>$2%>#
1%>%>2%$2%#
1(#
A>($4%%&&''''
A?(,/!#4
!
%2"(#
(#
1( (! 2/%.($+2/ 1)! ##
88.Infant’s medical record number:
89. Newborn Screening Number: _________________________________________
If Unknown check reason why
Religious Waiver |
|
|
90. Was the mother transferred to this facility for maternal medical or fetal indications for delivery? + " #
'
' 4
1/27/2017 |
PAGE 12 |
VERSION 29 INDIANA'S BIRTH WORKSHEET |
|