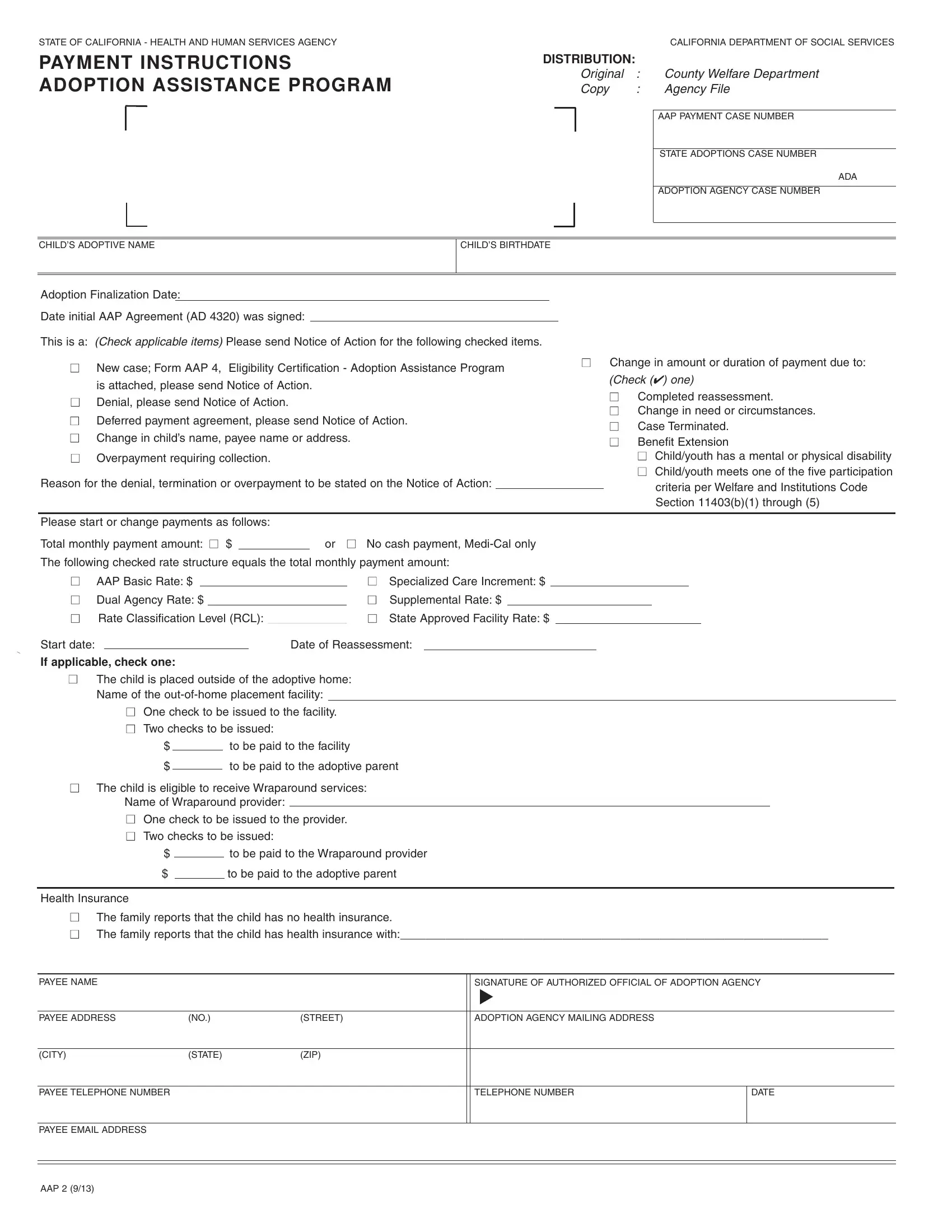
In the heart of the California Department of Social Services lies a crucial form that serves as the backbone for providing financial support to adoptive families, known as the Adoption Assistance Program (AAP) 2 form. This document outlines the necessary steps and required information crucial for processing payments under the Adoption Assistance Program. Designed with the welfare of adopted children in mind, it covers a wide array of payment instructions, including but not limited to, the initial setup of a new case, changes in the payment amount or duration, and cases of overpayment that require resolution. The form meticulously collects details such as the child’s adoptive name, birthdate, and the vital dates marking the adoption finalization and the signing of the initial AAP agreement. Furthermore, it accommodates various circumstances like changes in the child’s or payee's name, address, and eligibility for different rate structures based on the child’s needs, including basic, specialized care, and dual agency rates. It ensures adoptive parents are well-informed about their child’s eligibility for supplemental benefits, including health insurance, wraparound services, and specifies the method of payment distribution ensuring transparency and accountability at every step. This document is not just a form; it is a reflection of the state's commitment to facilitating seamless support to adoptive families, ensuring every child has the opportunity to thrive in a loving, supportive environment.
| Question | Answer |
|---|---|
| Form Name | California Form Aap 2 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | Deferred, medi, ADOPTIONS, placements |
STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AGENCY |
CALIFORNIA DEPARTMENT OF SOCIAL SERVICES |
PAYMENT INSTRUCTIONS ADOPTION ASSISTANCE PROGRAM
DISTRIBUTION:
Original |
: |
County Welfare Department |
Copy |
: |
Agency File |
|
|
|
|
|
AAP PAYMENT CASE NUMBER |
|
|
|
|
|
STATE ADOPTIONS CASE NUMBER |
|
|
ADA |
|
|
|
|
|
ADOPTION AGENCY CASE NUMBER |
|
|
|
CHILD’S ADOPTIVE NAME
CHILD’S BIRTHDATE
Adoption Finalization Date: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Date initial AAP Agreement (AD 4320) was signed: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
This is a: (Check applicable items) Please send Notice of Action for the following checked items. |
|
|
|
|
|
|
|
|||||||||||||||||
■ |
New case; Form AAP 4, Eligibility Certification - Adoption Assistance Program |
■ Change in amount or duration of payment due to: |
||||||||||||||||||||||
|
|
|
|
|
|
|
||||||||||||||||||
|
is attached, please send Notice of Action. |
|
|
|
|
|
|
|
|
|
(Check (✔) one) |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
■ Denial, please send Notice of Action. |
|
|
|
|
|
|
|
|
|
|
|
|
■ |
Completed reassessment. |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
■ Change in need or circumstances. |
||||||||||||
■ Deferred payment agreement, please send Notice of Action. |
|
|
||||||||||||||||||||||
|
|
■ |
Case Terminated. |
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
■ Change in child’s name, payee name or address. |
|
|
|
|
|
|
|
|
|
■ |
Benefit Extension |
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
■ |
Overpayment requiring collection. |
|
|
|
|
|
|
|
|
|
|
|
|
|
■ Child/youth has a mental or physical disability |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
■ Child/youth meets one of the five participation |
|||
Reason for the denial, termination or overpayment to be stated on the Notice of Action: |
|
|
|
|
criteria per Welfare and Institutions Code |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Section 11403(b)(1) through (5) |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Please start or change payments as follows: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Total monthly payment amount: ■ $ |
|
|
or ■ No cash payment, |
|
|
|
|
|
|
|
||||||||||||||
The following checked rate structure equals the total monthly payment amount: |
|
|
|
|
|
|
|
|||||||||||||||||
■ |
AAP Basic Rate: $ |
|
|
|
■ |
Specialized Care Increment: $ |
|
|
|
|
|
|
|
|
||||||||||
■ |
Dual Agency Rate: $ |
|
|
|
■ |
Supplemental Rate: $ |
|
|
|
|
|
|
|
|
||||||||||
■ Rate Classification Level (RCL): |
|
|
■ State Approved Facility Rate: $ |
|
|
|
|
|
|
|
|
|||||||||||||
Start date: |
|
|
|
|
|
|
|
Date of Reassessment: |
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
If applicable, check one:
■The child is placed outside of the adoptive home: Name of the
■One check to be issued to the facility.
■Two checks to be issued:
$ |
|
|
to be paid to the facility |
$ |
|
|
to be paid to the adoptive parent |
|
|
■The child is eligible to receive Wraparound services: Name of Wraparound provider:
■One check to be issued to the provider.
■Two checks to be issued:
$ |
|
to be paid to the Wraparound provider |
$ |
|
to be paid to the adoptive parent |
Health Insurance
■The family reports that the child has no health insurance.
■The family reports that the child has health insurance with:__________________________________________________________________
PAYEE NAME |
|
|
SIGNATURE OF AUTHORIZED OFFICIAL OF ADOPTION AGENCY |
|
|
|
|
|
▲ |
|
|
|
|
|
|
|
|
PAYEE ADDRESS |
(NO.) |
(STREET) |
ADOPTION AGENCY MAILING ADDRESS |
|
|
|
|
|
|
|
|
(CITY) |
(STATE) |
(ZIP) |
|
|
|
|
|
|
|
|
|
PAYEE TELEPHONE NUMBER |
|
|
TELEPHONE NUMBER |
DATE |
|
|
|
|
|
|
|
PAYEE EMAIL ADDRESS |
|
|
|
|
|
AAP 2 (9/13)