

Through the online PDF editor by FormsPal, it is possible to complete or modify form employer confirmation sample here. The editor is continually improved by our team, getting awesome features and growing to be greater. Starting is easy! All you have to do is stick to these easy steps below:
Step 1: Just click the "Get Form Button" in the top section of this site to access our form editing tool. There you'll find all that is required to work with your document.
Step 2: The tool offers the capability to change nearly all PDF forms in a variety of ways. Transform it by adding customized text, correct what is already in the file, and put in a signature - all at your disposal!
This form requires specific details; to guarantee accuracy and reliability, please pay attention to the suggestions below:
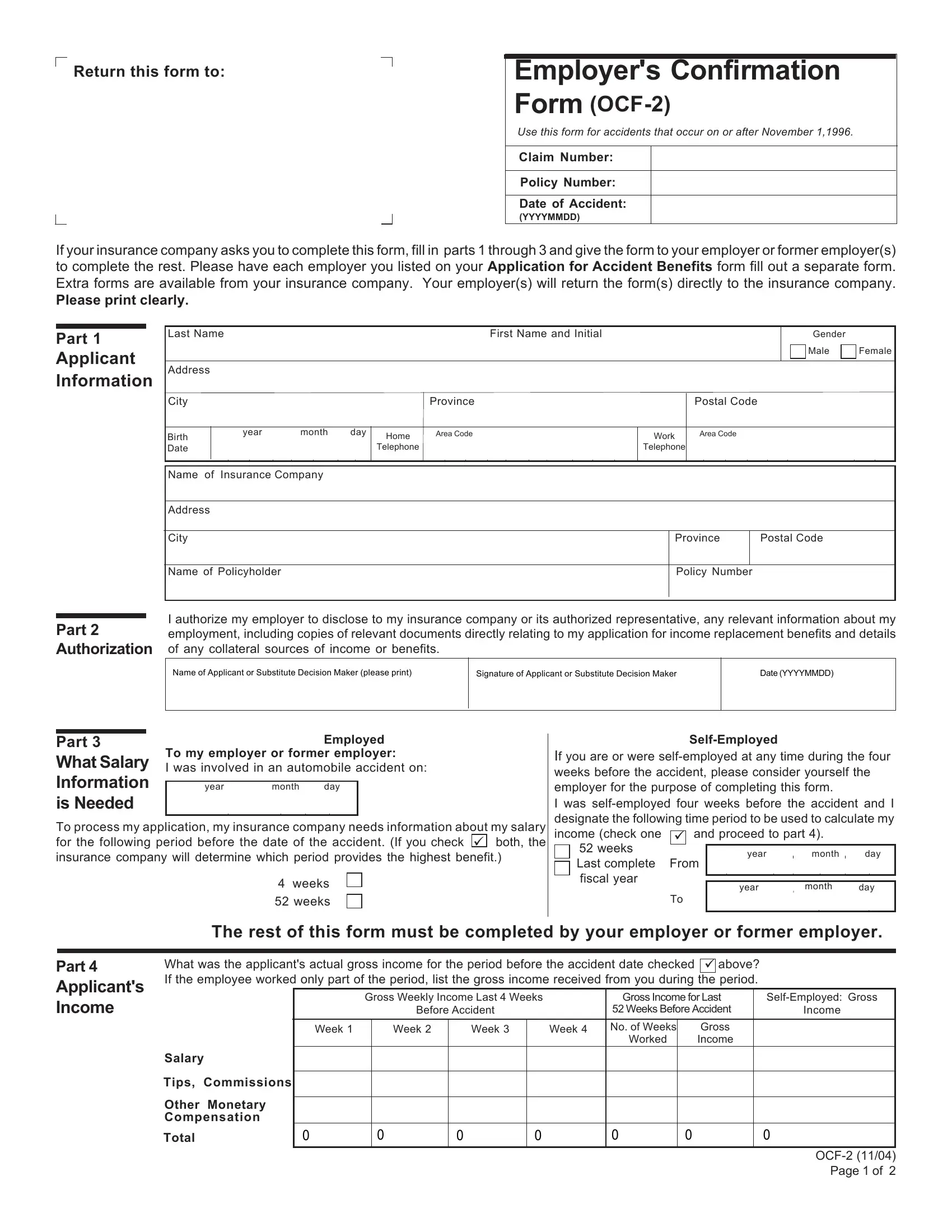
1. Start completing your form employer confirmation sample with a group of major blank fields. Get all of the required information and make certain there's nothing left out!
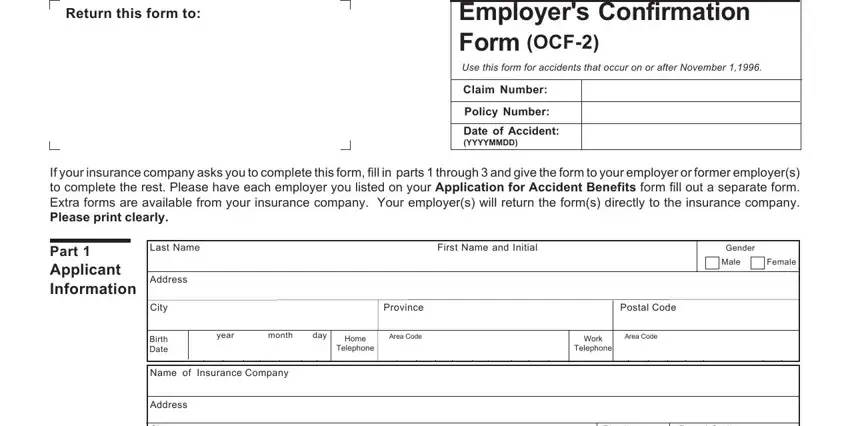
2. Once your current task is complete, take the next step – fill out all of these fields - City, Province, Postal Code, Name of Policyholder, Policy Number, Part Authorization of any, I authorize my employer to, Name of Applicant or Substitute, Signature of Applicant or, Date YYYYMMDD, Part What Salary Information is, To my employer or former employer, Employed, year, and month with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
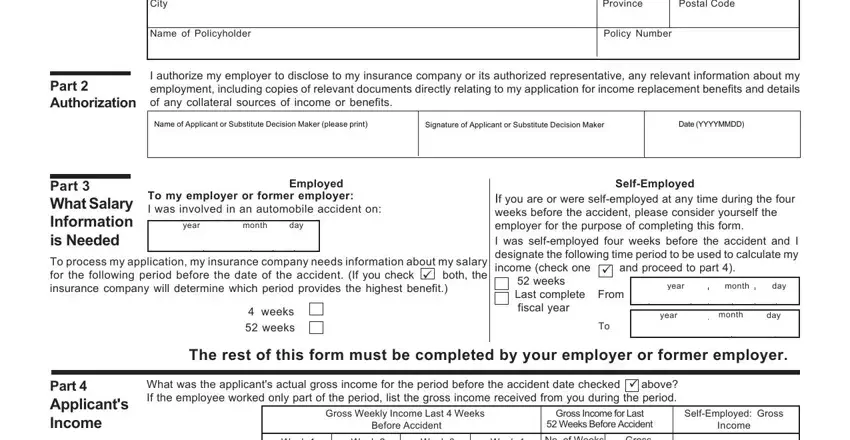
3. This next step is pretty simple, Week, Week, Week, Week, No of Weeks, Worked, Gross Income, Salary, Tips Commissions Other Monetary, and OCF Page of - these fields will need to be filled out here.
4. This next section requires some additional information. Ensure you complete all the necessary fields - Part Applicants Income contd, Part Other Benefits, Was the applicant absent from work, Yes Give details below, Are there any other types of, Yes Give details below, To your knowledge is the applicant, Income Continuation Benefit, Supplementary Medical, Sick Leave, Yes, Yes, Yes, Insurance Company, and Policy No - to proceed further in your process!
Be really mindful when filling out Sick Leave and Policy No, as this is where most users make errors.
5. And finally, the following last subsection is what you'll have to wrap up prior to using the form. The blank fields you're looking at are the next: Part Employment Details, additional sheets attached, Part Employer Information, Date of Employment, year, month, day, year month day, Latest Job Title, From, Last Date Worked, year, month, day, and Date of Return to Work if.
Step 3: Reread the information you've typed into the blanks and hit the "Done" button. Right after registering a7-day free trial account at FormsPal, you'll be able to download form employer confirmation sample or email it promptly. The PDF will also be readily available through your personal cabinet with your each and every change. We do not share or sell the details you enter while filling out forms at our site.