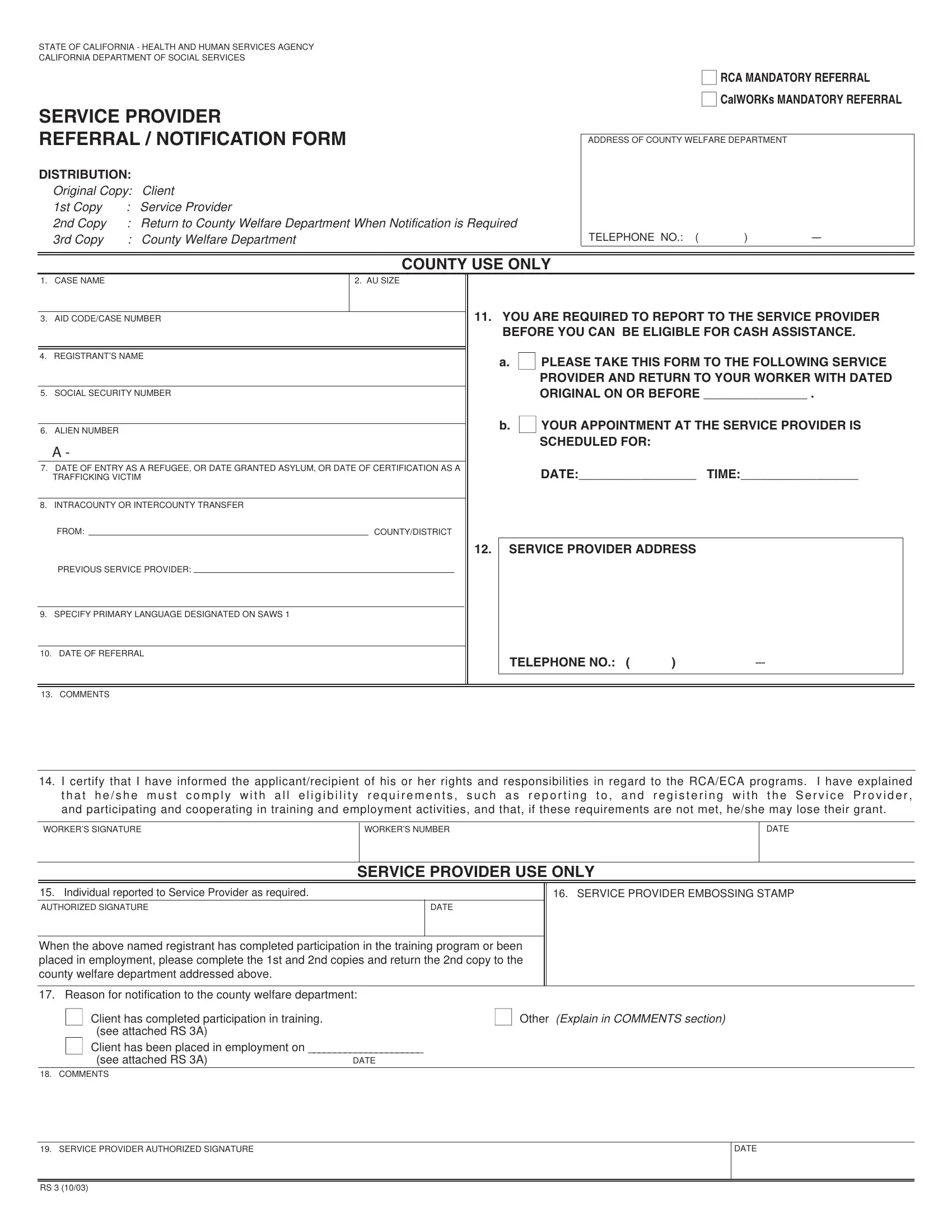
In California, navigating the bureaucratic process to attain social services can often feel labyrinthine, yet understanding the minutiae of these procedures is vital for those seeking assistance. This is particularly true for the RS 3 form, a critical document within the California Department of Social Services. Its primary purpose is to facilitate mandatory referrals within the RCA (Refugee Cash Assistance) and CalWORKs (California Work Opportunity and Responsibility to Kids) programs. Essentially, this form serves as a bridge between clients requiring services and the providers designated to offer those services. The distribution process is thoroughly detailed to ensure clarity and compliance; the original copy is retained by the client, while duplicates are distributed among the service provider and relevant county welfare departments. Aside from logistical details, such as the address and telephone number of the county welfare department, the form requires comprehensive identification and case information including the registrant’s name, social security number, alien number, and primary language. Furthermore, it mandates registrants to report to a designated service provider by a specified date to maintain eligibility for financial assistance. A section for comments allows personalized notes or explanations that might be pertinent to the individual’s case. Completing and returning this form in a timely manner is crucial, as non-compliance could result in the loss of benefits, making understanding each section’s requirements and deadlines of paramount importance for applicants.
| Question | Answer |
|---|---|
| Form Name | California Form Rs 3 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | cdss forms, 1st, 11b, EMBOSSING |