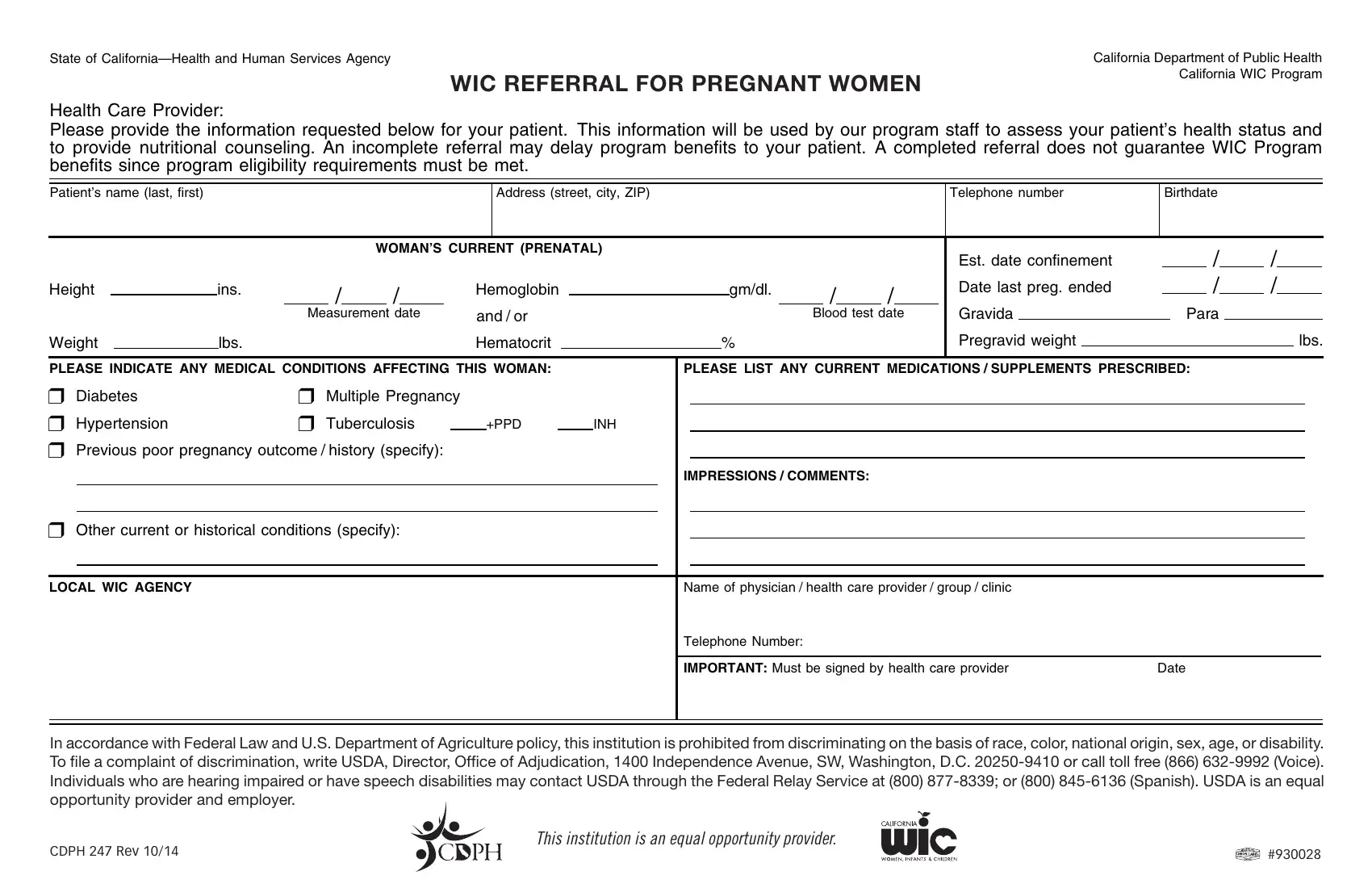
In the State of California, a crucial component of ensuring optimal health outcomes for both mothers and infants revolves around comprehensive nutritional and health support services, prominently facilitated through the California Women, Infants, and Children (WIC) Program. This program meticulously designed by the California Department of Public Health, seeks to bridge the gap in nutritional counseling and support for pregnant, breastfeeding, and postpartum women, along with infants facing health risks due to nutrition-related issues. The WIC referral forms, differentiated for pregnant and postpartum/breastfeeding women, constitute a foundational step in this process, requiring healthcare providers to furnish detailed patient information including health status, medical conditions, and prescribed medications or supplements. This meticulous documentation aims to empower WIC program staff to conduct an informed assessment of the patient's health needs and align program benefits effectively. However, it is emphasized that completion of the referral form does not automatically ensure eligibility for WIC benefits, as patients must meet specific program criteria. Moreover, these forms underscore the State’s commitment to equality and non-discrimination in service provision, adhering to federal laws that prohibit discrimination based on race, color, national origin, sex, age, or disability, thereby enshrining principles of inclusivity and equal opportunity in accessing health support services.
| Question | Answer |
|---|---|
| Form Name | California Wic Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | california wic form, ca wic form pdf, ca wic referral, ca wic form |
State of
WIIC REFERRAL FORPREGNANT WOMENAN
Health Care Provider:
California Department of Public Health
CALIFORNIA WIC Program
Please provide the information requested below for your patient. This information will be used by our program staff to assess your patient’s health status and to provide nutritional counseling. An incomplete referral may delay program benefits to your patient. A completed referral does not guarantee WIC Program benefits since program eligibility requirements must be met.
Patient’s name (last, first)
Address (street, city, ZIP)
Telephone number
Birthdate
WOMAN’S CURRENT (PRENATAL)
Height |
|
|
ins. |
|
/ |
|
/ |
|
Hemoglobin |
|
|
gm/dl. |
|
/ |
|
/ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
Measurement date |
and / or |
|
|
|
Blood test date |
|||||||||
Weight |
|
|
lbs. |
|
|
|
|
|
Hematocrit |
|
|
% |
|
|
|
|
|
|
Est. date confinement |
|
|
/ |
|
|
/ |
|
|
||
Date last preg. ended |
|
|
/ |
|
|
/ |
|
|
||
Gravida |
|
|
|
Para |
|
|
|
|
||
Pregravid weight |
|
|
|
|
|
|
|
|
lbs. |
|
PLEASE INDICATE ANY MEDICAL CONDITIONS AFFECTING THIS WOMAN: |
PLEASE LIST ANY CURRENT MEDICATIONS / SUPPLEMENTS PRESCRIBED: |
❒ Diabetes |
❒ Multiple Pregnancy |
|
|
|
|
|
||
❒ Hypertension |
❒ Tuberculosis |
|
+PPD |
|
INH |
|
||
❒ Previous poor pregnancy outcome / history (specify): |
|
|
|
|
|
|||
|
|
|
|
|
|
|
IMPRESSIONS / COMMENTS: |
|
❒Other current or historical conditions (specify):
LOCAL WIC AGENCY |
Name of physician / health care provider / group / clinic |
|
|
Telephone Number: |
|
|
|
|
|
IMPORTANT: Must be signed by health care provider |
Date |
In accordance with Federal Law and U.S. Department of Agriculture policy, this institution is prohibited from discriminating on the basis of race, color, national origin, sex, age, or disability. To file a complaint of discrimination, write USDA, Director, Office of Adjudication, 1400 Independence Avenue, SW, Washington, D.C.
This institution is an equal opportunity provider.
CDPH 247 REV 10/14 |
#930028 |
|
State of |
CALIFORNIA Department of Public Health |
WIC REFERRAL FOR POSTPARTUM/BREASTFEEDINGI WOMENAN |
CaliforniaWICProgram |
|
Health Care Provider:
Please provide the information requested below for your patient. This information will be used by our program staff to assess your patient’s health status and to provide nutritional counseling. An incomplete referral may delay program benefits to your patient. A completed referral does not guarantee WIC Program benefits since program eligibility requirements must be met.
Patient’s name (last, first)
Address (street, city, ZIP code)
Telephone number
Birthdate
WOMAN’S CURRENT (After Delivery)
Height |
|
|
|
ins. |
|
/ |
|
/ |
|
|
|
|
|
|
|
|
|
||
Weight |
|
|
lbs. |
Measurement date |
|||||
Hemoglobin |
|
gm/dl. |
|
/ |
|
/ |
|
||
and/or |
|
|
|
|
|||||
|
Blood test date |
||||||||
Hematocrit |
|
% |
|||||||
|
|
|
|
|
|
||||
|
|
|
|
PREGNANCY OUTCOME |
|
|
|
/ |
|
|
/ |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Preterm |
Sm. Gest. |
Fetal |
|
|
|
|
Delivery date |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
(37 wks.) |
Age |
Loss |
Stillbirth |
|
|
|
|
|
|
|
|
|
|
|
|
1. |
❒ |
❒ |
❒ |
❒ |
❒ |
|
|
|
|
|
|
|
|
|
|
|
Sex |
|
Birth weight |
|
|
Birth length |
|||||||||||
|
|
|
|
|
|
|
|
|
||||||||
2. |
❒ |
❒ |
❒ |
❒ |
❒ |
|
|
|
|
|
|
|
|
|
|
|
Please describe any medical conditions affecting the infant(s): |
Sex |
|
Birth weight |
|
|
Birth length |
||||||||||
PLEASE INDICATE ANY MEDICAL CONDITIONS AFFECTING THIS WOMAN. |
PLEASE LIST ANY CURRENT MEDICATIONS/SUPPLEMENTS PRESCRIBED: |
❒ |
|
❒ Other conditions occurring during this pregnancy or delivery |
|
|
|
|
|||||||
❒ Diabetes |
|
(specify): |
|
|
|
|
|
|
|||||
❒ Hypertension |
|
|
|
|
|
IMPRESSIONS / COMMENTS: |
|
|
|
||||
❒ Tuberculosis |
|
❒ Other current or historical medical conditions (specify): |
|
|
|
|
|||||||
|
|
+PPD |
|
INH |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
LOCAL WIC AGENCY |
|
|
|
|
Name of physician / health care provider / group / clinic |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
Telephone number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
IMPORTANT: Must be signed by health care provider |
Date |
|||
In accordance with Federal Law and U.S. Department of Agriculture policy, this institution is prohibited from discriminating on the basis of race, color, national origin, sex, age, or disability. To file a complaint of discrimination, write USDA, Director, Office of Adjudication, 1400 Independence Avenue, SW, Washington, D.C.
This institution is an equal opportunity provider.
CDPH 247 REV 10/14 |
#930028 |
|