
Handling PDF forms online is a breeze with this PDF editor. Anyone can fill out medications here effortlessly. The tool is consistently upgraded by us, receiving handy features and growing to be better. In case you are looking to get going, this is what it takes:
Step 1: Just click the "Get Form Button" in the top section of this page to open our pdf form editing tool. Here you'll find all that is necessary to fill out your file.
Step 2: This editor will let you work with almost all PDF forms in a range of ways. Change it by writing your own text, adjust what's originally in the PDF, and put in a signature - all at your convenience!
This PDF form needs some specific information; in order to guarantee accuracy, remember to bear in mind the suggestions below:
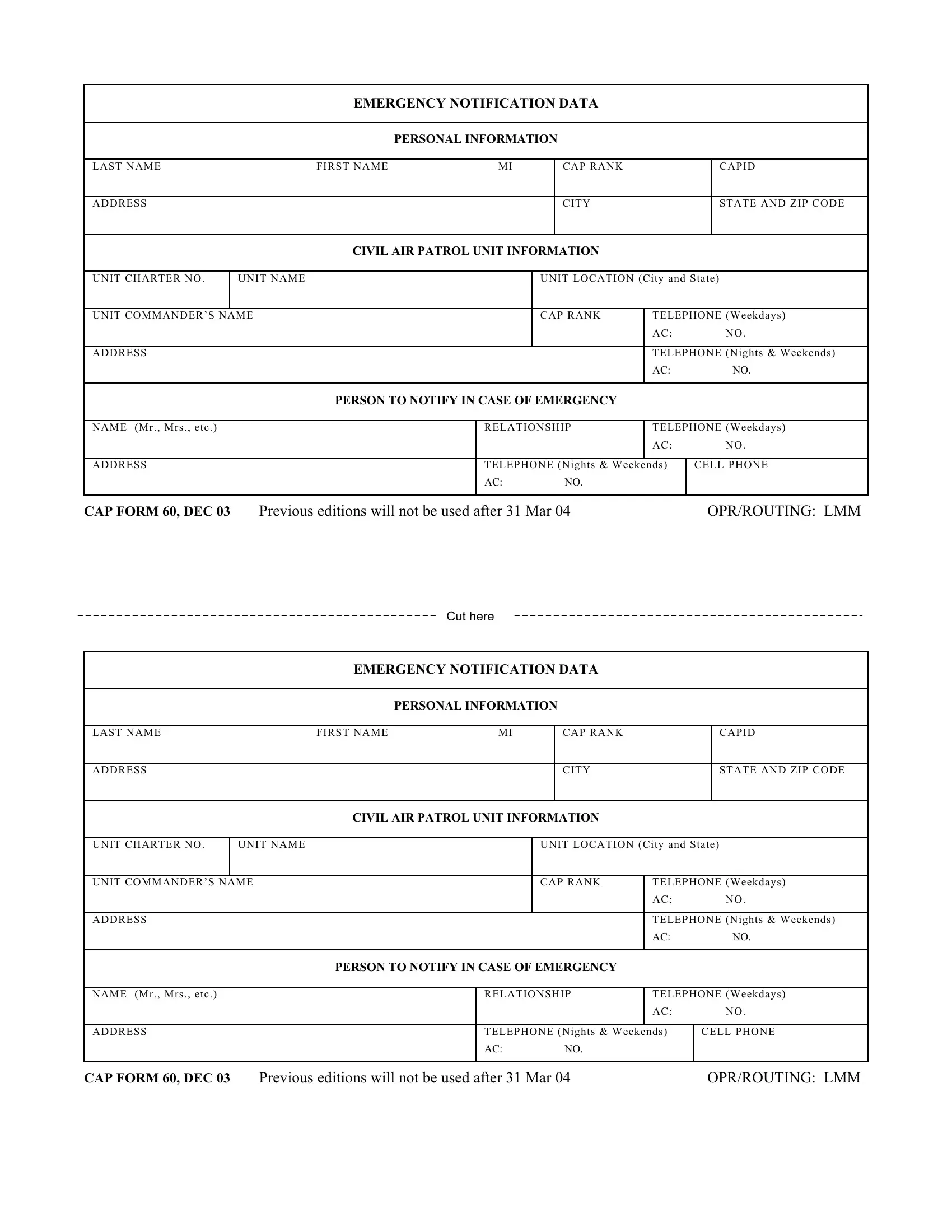
1. The medications involves particular details to be typed in. Ensure the subsequent blank fields are filled out:
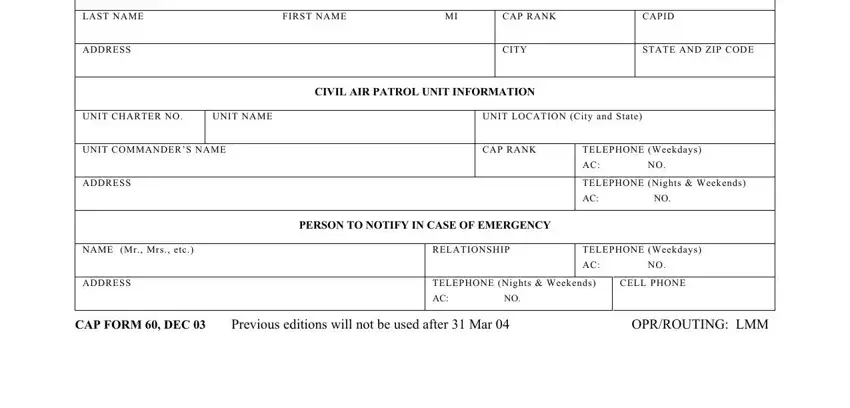
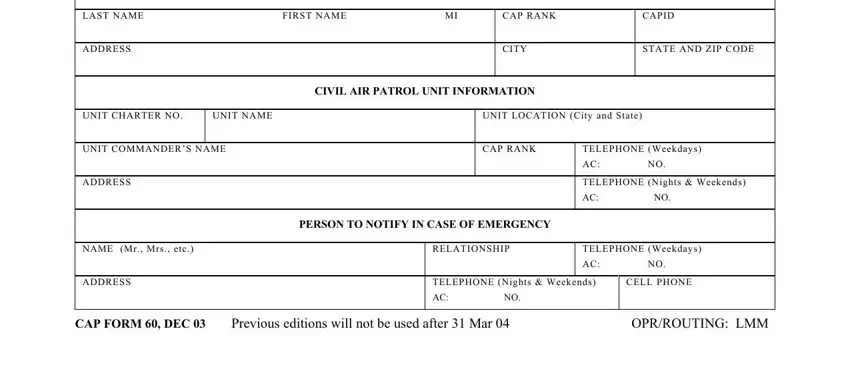
2. Once your current task is complete, take the next step – fill out all of these fields - FIRST NAME, CAP RANK, CITY, CAPID, STATE AND ZIP CODE, CIVIL AIR PATROL UNIT INFORMATION, UNIT LOCATION City and State, CAP RANK, TELEPHONE Weekdays AC NO, TELEPHONE Nights Weekends AC NO, PERSON TO NOTIFY IN CASE OF, RELATIONSHIP, TELEPHONE Weekdays AC NO, TELEPHONE Nights Weekends AC NO, and CELL PHONE with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. The third step is straightforward - fill out all of the empty fields in EMERGENCY MEDICAL DATA, PERSONAL PHYSICIAN, PHYSICIANS ADDRESS, PHONE, CITY, BLOOD TYPE, PERTINENT MEDICAL DATA Allergies, and CAP FORM DEC REVERSE in order to finish this part.
You can potentially get it wrong while completing the EMERGENCY MEDICAL DATA, consequently make sure that you reread it before you submit it.
4. Filling in EMERGENCY MEDICAL DATA, PERSONAL PHYSICIAN, PHYSICIANS ADDRESS, PHONE, CITY, BLOOD TYPE, PERTINENT MEDICAL DATA Allergies, and CAP FORM DEC REVERSE is essential in this next form section - make certain that you don't rush and fill in each empty field!
Step 3: Soon after rereading your fields and details, click "Done" and you are done and dusted! After creating afree trial account with us, you will be able to download medications or send it through email without delay. The PDF file will also be readily available from your personal account with your every change. With FormsPal, you're able to complete forms without being concerned about information breaches or records being shared. Our protected software makes sure that your personal data is stored safely.