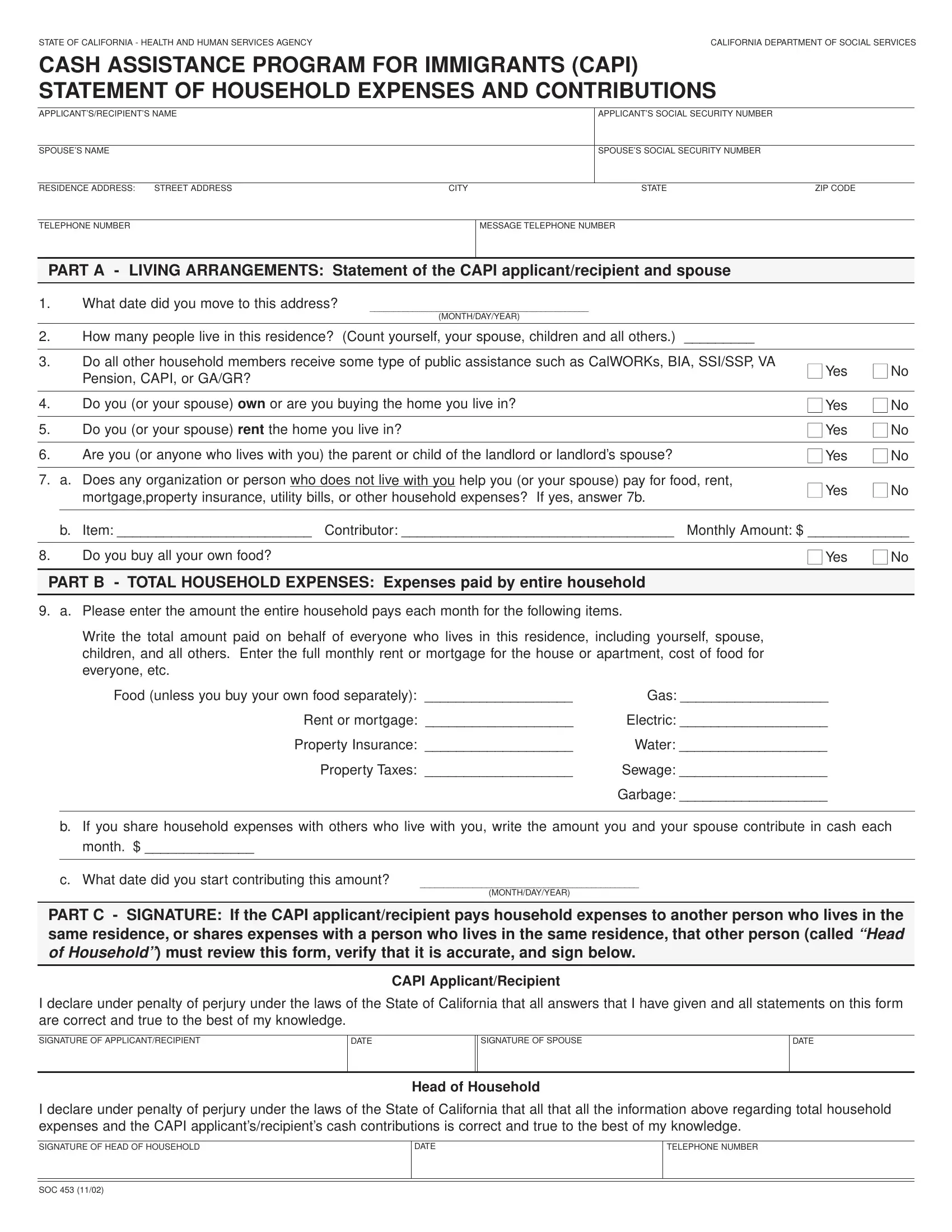
Navigating the complexities of financial assistance programs can often seem daunting, but understanding the necessary forms and documentation is a crucial step towards accessing benefits. Among these, the CAPI Statement of Household Expenses and Contributions form, officially known as SOC 453, plays a vital role for immigrants in California seeking cash assistance. Managed by the California Department of Social Services, this form is designed to capture detailed information about an applicant's living situation, household members, and financial contributions towards household expenses. Applicant's and their spouse's personal information, including social security numbers and residence details, form the basis of this document. The form delves into specifics such as the number of people living in the residence, their receipt of any public assistance, homeownership or rental status, and any external financial support for household expenses. Additionally, it requires a comprehensive account of monthly household expenses, including rent or mortgage, utilities, food, and more, to understand the financial dynamics of the household. Accurate and truthful completion of this form, verified under penalty of perjury, is necessary for the evaluation of a CAPI application. The importance of this form cannot be overstated, as it ensures that aid is appropriately allocated to those in need, reflecting the state’s commitment to supporting its immigrant population.
| Question | Answer |
|---|---|
| Form Name | CAPI Form SOC 453 |
| Form Length | 1 pages |
| Fillable? | Yes |
| Fillable fields | 37 |
| Avg. time to fill out | 7 min 43 sec |
| Other names | mortgageproperty, capi calm soc 453 sp form, CAPI, forms soc 453 |
STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AGENCYCALIFORNIA DEPARTMENT OF SOCIAL SERVICES
CASH ASSISTANCE PROGRAM FOR IMMIGRANTS (CAPI) STATEMENT OF HOUSEHOLD EXPENSES AND CONTRIBUTIONS
APPLICANT’S/RECIPIENT’S NAME |
|
|
|
|
|
APPLICANT’S SOCIAL SECURITY NUMBER |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SPOUSE’S NAME |
|
|
|
|
|
|
|
SPOUSE’S SOCIAL SECURITY NUMBER |
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
RESIDENCE ADDRESS: |
|
STREET ADDRESS |
|
CITY |
|
|
|
STATE |
|
|
ZIP CODE |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TELEPHONE NUMBER |
|
|
|
|
|
MESSAGE TELEPHONE NUMBER |
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PART A - LIVING ARRANGEMENTS: Statement of the CAPI applicant/recipient and spouse
1. |
What date did you move to this address? |
______________________________________________ |
|
|
|
|
|
(MONTH/DAY/YEAR) |
|
|
|
|
|
|
|
|
|
2. |
How many people live in this residence? |
(Count yourself, your spouse, children and all others.) |
_________ |
|
|
|
|
|
|
||
3. |
Do all other household members receive some type of public assistance such as CalWORKs, BIA, SSI/SSP, VA |
■ Yes |
■ No |
||
|
Pension, CAPI, or GA/GR? |
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
4. |
Do you (or your spouse) own or are you buying the home you live in? |
|
■ Yes |
■ No |
|
|
|
|
|
|
|
5. |
Do you (or your spouse) rent the home you live in? |
|
■ Yes |
■ No |
|
|
|
|
|
|
|
6. |
Are you (or anyone who lives with you) the parent or child of the landlord or landlord’s spouse? |
|
■ Yes |
■ No |
|
|
|
|
|
||
7. |
a. Does any organization or person who does not live with you help you (or your spouse) pay for food, rent, |
■ Yes |
■ No |
||
|
mortgage,property insurance, utility bills, or other household expenses? If yes, answer 7b. |
|
|||
|
|
|
|
||
|
|
|
|||
|
b. Item: _________________________ Contributor: ___________________________________ |
Monthly Amount: $ _____________ |
|||
|
|
|
|
|
|
8. |
Do you buy all your own food? |
|
|
■ Yes |
■ No |
|
|
|
|
|
|
PART B - TOTAL HOUSEHOLD EXPENSES: Expenses paid by entire household
9. a. Please enter the amount the entire household pays each month for the following items.
Write the total amount paid on behalf of everyone who lives in this residence, including yourself, spouse, children, and all others. Enter the full monthly rent or mortgage for the house or apartment, cost of food for everyone, etc.
|
Food (unless you buy your own food separately): ___________________ |
Gas: ___________________ |
|
|
Rent or mortgage: ___________________ |
Electric: ___________________ |
|
|
Property Insurance: ___________________ |
Water: ___________________ |
|
|
Property Taxes: ___________________ |
Sewage: ___________________ |
|
|
|
Garbage: ___________________ |
|
|
|
|
|
|
|
|
|
b.If you share household expenses with others who live with you, write the amount you and your spouse contribute in cash each month. $ ______________
c. What date did you start contributing this amount?
______________________________________________
(MONTH/DAY/YEAR)
PART C - SIGNATURE: If the CAPI applicant/recipient pays household expenses to another person who lives in the same residence, or shares expenses with a person who lives in the same residence, that other person (called “Head of Household”) must review this form, verify that it is accurate, and sign below.
CAPI Applicant/Recipient
I declare under penalty of perjury under the laws of the State of California that all answers that I have given and all statements on this form are correct and true to the best of my knowledge.
SIGNATURE OF APPLICANT/RECIPIENT
DATE
SIGNATURE OF SPOUSE
DATE
Head of Household
I declare under penalty of perjury under the laws of the State of California that all that all the information above regarding total household expenses and the CAPI applicant’s/recipient’s cash contributions is correct and true to the best of my knowledge.
SIGNATURE OF HEAD OF HOUSEHOLD
DATE
TELEPHONE NUMBER
SOC 453 (11/02)