
By using the online PDF editor at FormsPal, you can fill in and edit the CAPI Form SOC 814 directly in your browser. Our editor is updated regularly based on user feedback to keep it practical and easy to use. Getting started is simple. Follow the steps below:
Steps to Fill Out the CAPI Form SOC 814 Online
Step 1: Click the "Get Form" button above to open the CAPI Form SOC 814 in the FormsPal PDF editor.
Step 2: Use the editor to complete, customize, and review all required fields in the CAPI application. You can add text, adjust existing entries, add graphics, and sign the document electronically.
This PDF form requires specific details about your personal circumstances, immigration status, and financial situation. Keep the following guidelines in mind as you complete each section:
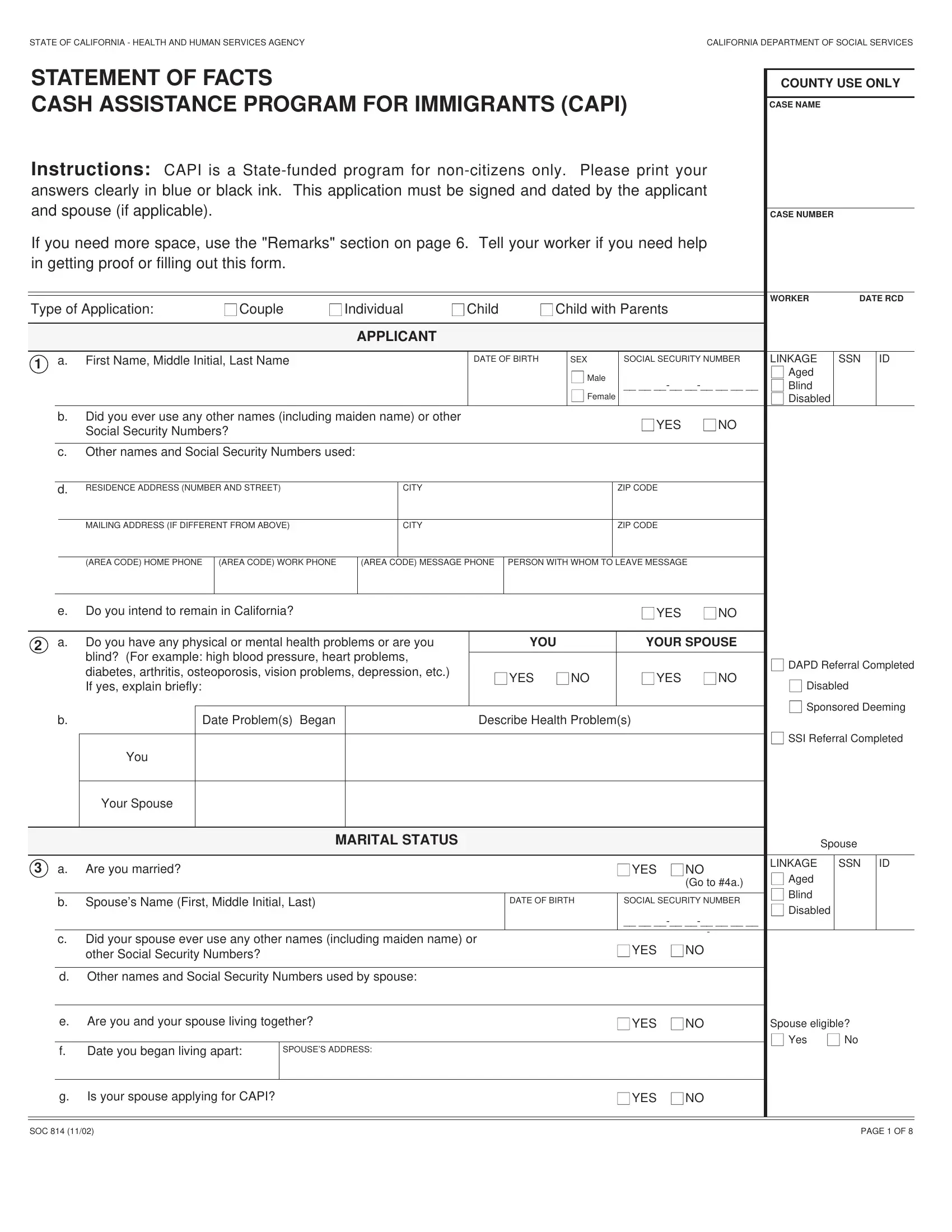
1. Complete the opening section of the CAPI SOC 814 accurately, paying close attention to all required fields:
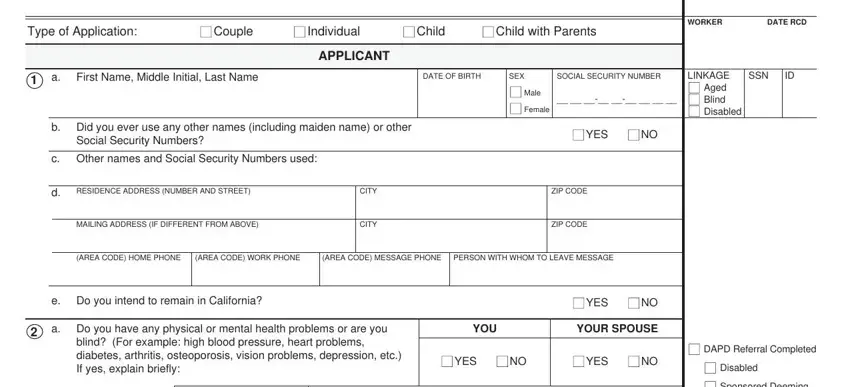
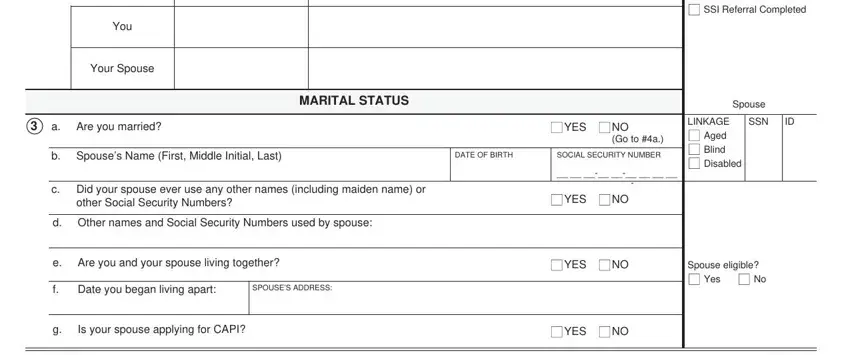
2. After completing the first section, enter the essential details including Date Problems Began, Health Problems Description, Marital Status, Spouse Name and Date of Birth, Social Security Number, and SSI Referral Completed.
Double-check your personal information in this section before moving on to avoid errors in the CAPI application.
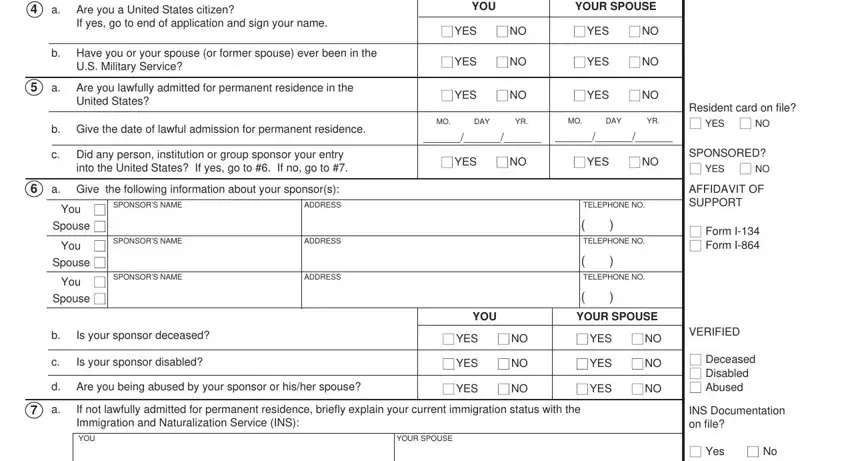
3. Complete the citizenship and immigration status section, including US Military Service history, lawful admission date, Alien Registration Number, and sponsor information. This section is critical for determining CAPI eligibility based on your immigration status.
4. The residency section of the CAPI SOC 814 gathers information about where you live. Complete all fields including US Resident status, Passport details, Alien Registration Number, Port of Entry, and your current living arrangement details.
5. The final section covers your living situation, need for home assistance, cooking facilities, and available support. Complete all required fields about your current living arrangement before submitting the CAPI Form SOC 814.
Step 3: Review all entries for accuracy, then click "Done" to complete the task. With a free FormsPal account, you can download the CAPI Form SOC 814 or send it via email right away. Your information stays private and secure throughout the process.
Frequently Asked Questions About the CAPI Form SOC 814
What is the CAPI Form SOC 814 used for?
The CAPI Form SOC 814 is the official statement of facts required to apply for the California Cash Assistance Program for Immigrants. It collects personal, immigration, income, and residency information to assess CAPI eligibility for non-citizen applicants.
Who can apply for CAPI benefits using this form?
Eligible applicants must be non-citizens who are 65 or older, blind, or disabled, who reside in California, and whose income and resources fall within the CAPI program limits. Applicants must also be lawfully admitted and ineligible for SSI or other federal benefit programs.
Where do I submit the completed CAPI application?
Submit your completed CAPI Form SOC 814 to your county Department of Social Services office in California. You may also need to attend an in-person CAPI eligibility interview at the county office.
What documents do I need for the CAPI application?
You will typically need to provide proof of identity, immigration status documents, California residency verification, income records, and information about your financial resources when applying through the CAPI program.
Related California Social Services Forms
If you need other California social services forms as part of your CAPI application, these related forms may also be helpful:
- CAPI Form SOC 453 - additional CAPI documentation for California immigrants
- California Form SOC 295 - California Department of Social Services form
- California Form SOC 450 - California social services application
- Application for Financial Assistance - general financial assistance application for eligible residents