
You can fill out CAPI Form SOC 453 completely online using FormsPal's free PDF editor. No software installation is required. Simply open the document in your browser, complete each section, then sign and download your finished application for free.
Steps to Fill Out CAPI Form SOC 453
Follow these steps to complete the California household expenses statement online:
Step 1: Click the "Get Form" button at the top of this page to open the SOC 453 in FormsPal's online editor.
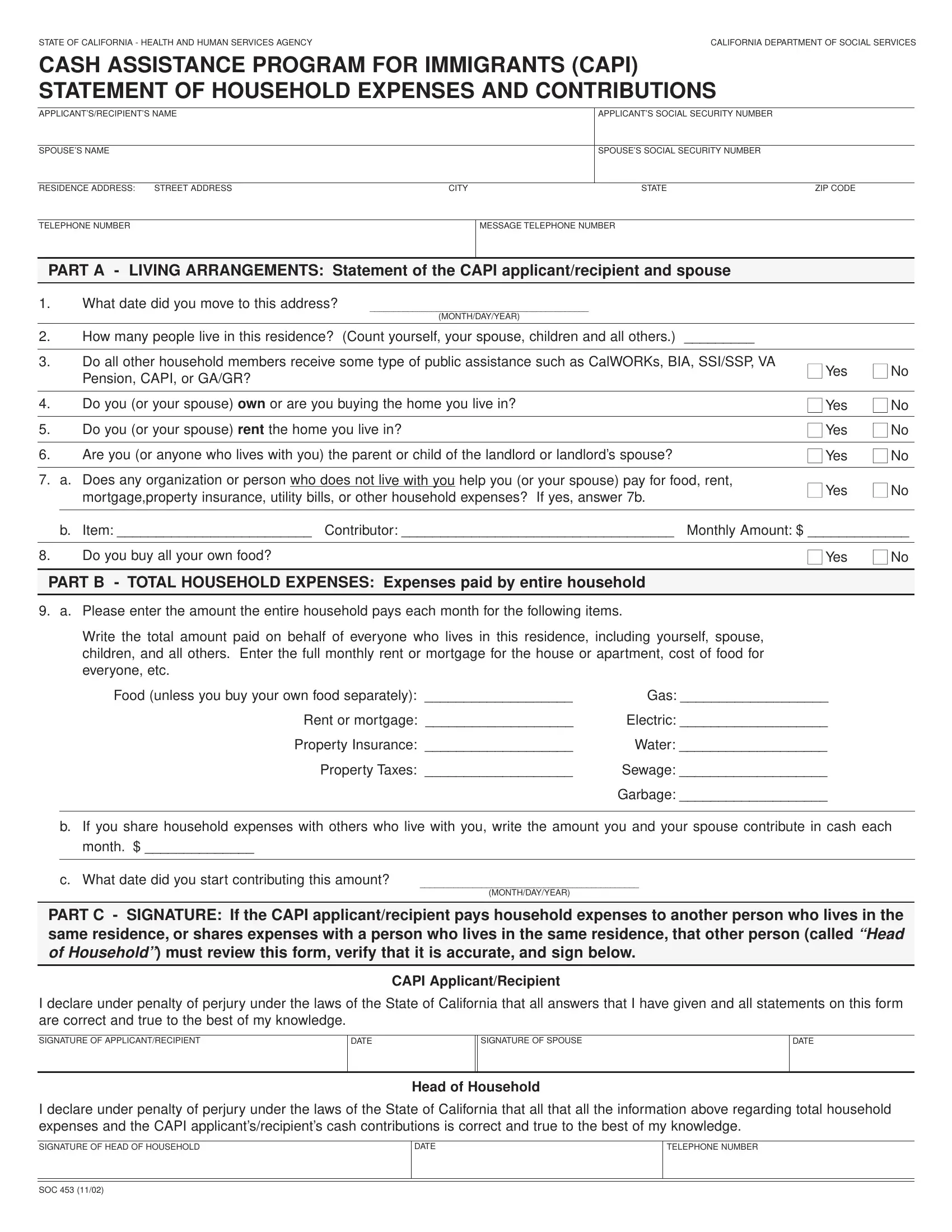
Step 2: Enter your personal information in Section 1. Include your full name, date of birth, address, social security number, and immigration status. Provide matching details for your spouse if applicable.
Step 3: Complete the household information section. List all individuals living in your residence, note whether anyone receives public assistance, and indicate whether you own or rent your home.
Step 4: Report your monthly household expenses in full. Include rent or mortgage payments, utility costs, food, and all other regular household costs. List any contributions received from family members or outside contributors toward these expenses.
Step 5: Review all entries carefully before signing. The document must be signed under penalty of perjury, confirming all information provided is accurate and complete. Use the digital signature tool in FormsPal's editor to sign the completed document.
Step 6: Download the completed SOC 453 as a PDF file. Bring the signed document to your local county social services office or submit it as directed by your caseworker during the CAPI application process.
Common Questions About CAPI Form SOC 453
What is the CAPI SOC 453 used for?
CAPI Form SOC 453 is a Statement of Household Expenses and Contributions used in California's Cash Assistance Program for Immigrants. It documents your household's financial situation so the California Department of Social Services can determine your benefit eligibility and calculate the appropriate payment amount.
Who needs to complete the SOC 453?
Immigrants applying for or renewing cash assistance through the CAPI program in California must complete this document. Your spouse may also need to provide information if they share household expenses with you. Contact your caseworker if you have questions about who should sign the application.
Where do I submit the completed document?
Submit the completed CAPI Form SOC 453 to your local county social services office. Contact your county's department of public social services for the correct submission address and any additional documentation requirements for the CAPI program.
Is there a cost to complete this document online?
No. You can complete and download the CAPI SOC 453 at no cost using FormsPal's online PDF editor. There are no fees for filling out, signing, or downloading the finished document.
Related California Assistance Documents
If you are navigating the CAPI application process, these related documents may also be needed:
- CAPI Form SOC 814 - Use this to report changes in your household status and continue receiving CAPI program benefits
- Financial Assistance Application - General financial assistance application for California residents who need additional support
- Household Employer Document - For individuals who employ household workers and need to report related expenses