
By using the online PDF tool by FormsPal, you can fill in or edit DAPD here. To have our editor on the cutting edge of practicality, we work to implement user-driven capabilities and improvements on a regular basis. We're at all times looking for suggestions - play a pivotal role in reshaping the way you work with PDF files. Getting underway is simple! All you need to do is follow these simple steps down below:
Step 1: Click on the "Get Form" button above on this webpage to get into our PDF editor.
Step 2: Using this handy PDF editor, you can accomplish more than merely complete forms. Try all of the functions and make your documents seem great with customized textual content added, or adjust the original input to perfection - all comes along with an ability to add any type of graphics and sign the file off.
This PDF doc will require specific details; to ensure consistency, you should bear in mind the next guidelines:
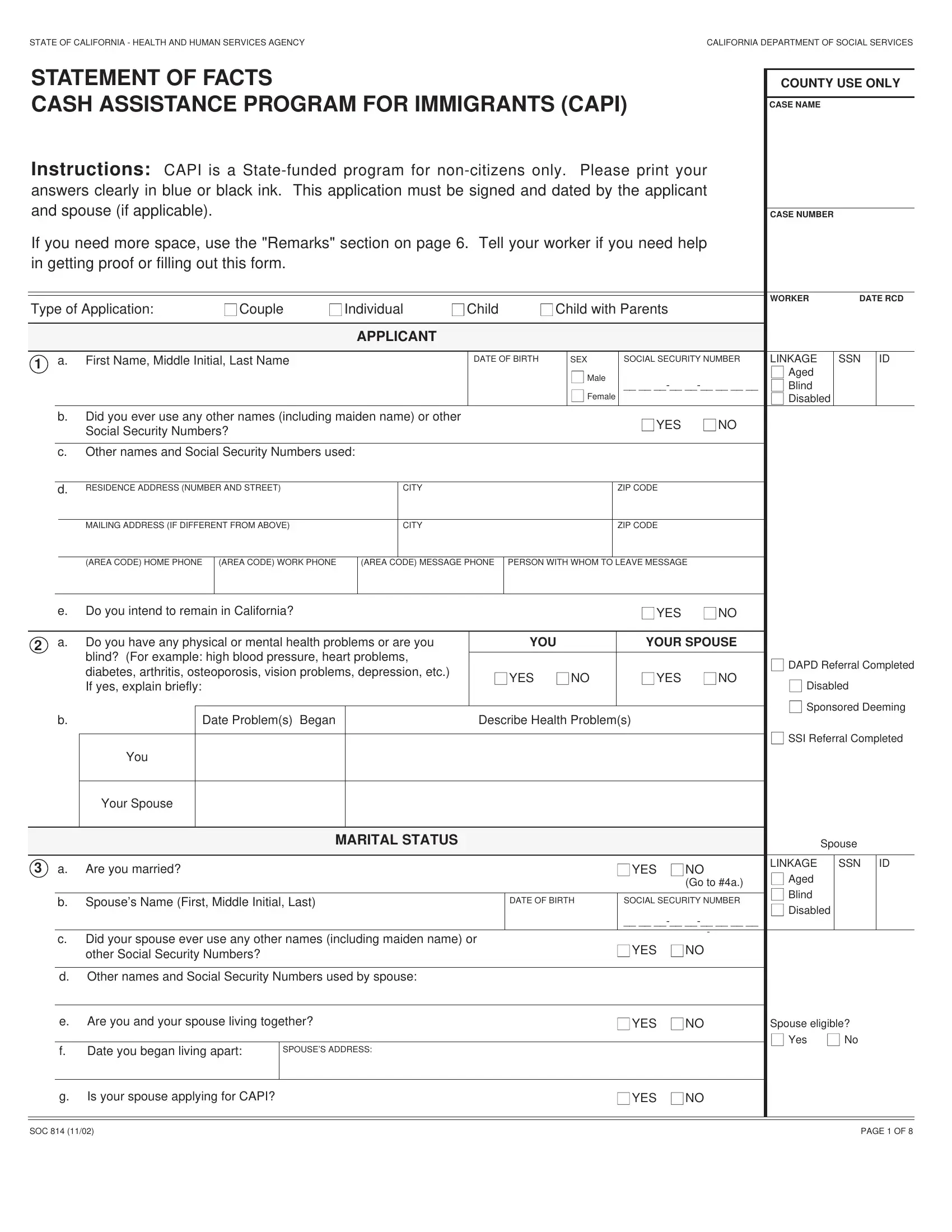
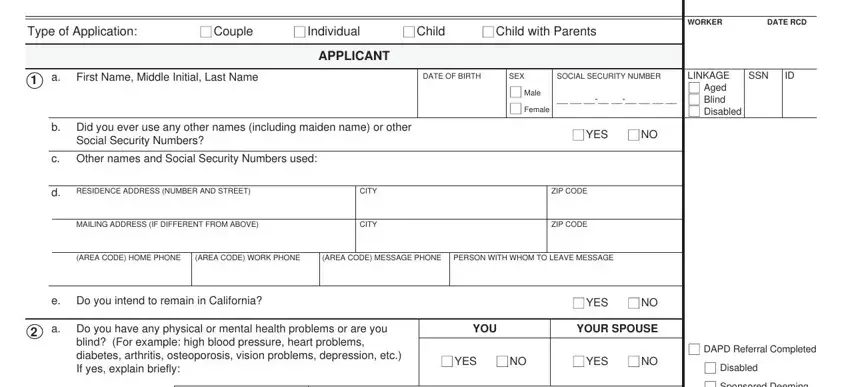
1. It's vital to complete the DAPD accurately, hence be careful while filling out the parts including all these blanks:
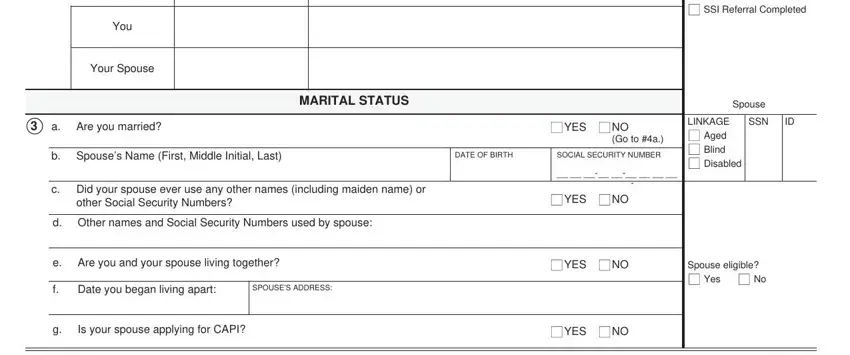
2. Just after filling in the last section, go on to the next part and enter the essential particulars in these blank fields - Date Problems Began, Describe Health Problems, You, Your Spouse, Are you married, MARITAL STATUS, YES, Go to a, Spouses Name First Middle Initial, DATE OF BIRTH, SOCIAL SECURITY NUMBER, Did your spouse ever use any other, d Other names and Social Security, YES, and SSI Referral Completed.
It is easy to make a mistake while filling in your You, consequently make sure you look again before you decide to finalize the form.
3. Completing Are you a United States citizen If, b Have you or your spouse or, US Military Service, Are you lawfully admitted for, YOU, YOUR SPOUSE, YES, YES, YES, YES, YES, YES, b Give the date of lawful, Did any person institution or, and MO DAY YR is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
4. This next section requires some additional information. Ensure you complete all the necessary fields - US Resident, Yes, Passport viewed and copy on file, Month aid begins, Through what date will INS allow, What is your Alien Registration, What was your Port of Entry, RESIDENCY, YOU, YOUR SPOUSE, Are you hiding or running from, or a parole or probation violation, YOU, YOUR SPOUSE, and YES - to proceed further in your process!
5. The very last notch to conclude this form is pivotal. Make sure you fill in the necessary fields, and this includes Check the applicable block to show, Room commercial establishment, Nursing Home, Jail, Shelter for Battered Women Other, a Do you need assistance in your, b Do you have adequate cooking and, available, YOU, YOUR SPOUSE, YES, YES, YES, YES, and IHSS Referral NMOHC, before using the pdf. If not, it might produce an unfinished and possibly unacceptable document!
Step 3: Ensure that the information is accurate and then just click "Done" to conclude the task. Right after getting afree trial account at FormsPal, it will be possible to download DAPD or send it via email without delay. The PDF form will also be available through your personal cabinet with your every single edit. FormsPal ensures your information privacy by having a secure method that in no way saves or shares any sort of personal information used. Rest assured knowing your paperwork are kept safe any time you work with our tools!