


Should you would like to fill out carefirst enrollment eft, it's not necessary to install any sort of applications - just try our PDF tool. To keep our tool on the cutting edge of practicality, we aim to put into operation user-oriented features and improvements on a regular basis. We're at all times looking for feedback - join us in reshaping how you work with PDF docs. Getting underway is effortless! All you have to do is take the following easy steps directly below:
Step 1: Access the PDF form in our editor by hitting the "Get Form Button" above on this page.
Step 2: This editor gives you the opportunity to modify your PDF in a range of ways. Improve it by including your own text, adjust original content, and put in a signature - all manageable in minutes!
It is actually simple to complete the pdf adhering to this practical guide! Here is what you need to do:
1. Whenever submitting the carefirst enrollment eft, make certain to complete all of the important fields in the associated section. This will help expedite the work, enabling your information to be handled swiftly and accurately.
2. Your next step would be to submit all of the following blank fields: Account Number Linkage to Provider, SUBMISSION INFORMATION, Checking, Savings, Provider Tax Identification Number, National Provider Identifier NPI, Reason for Submission select one, New Enrollment, Change Enrollment, Cancel Enrollment, Include with Enrollment Submission, Voided Check, Bank Letter, Attach a voided check to this space, and Attach a copy of a bank letter.
3. The following portion is about I we certify that I am a duly, Authorized Signature, Submission Date, Requested EFT StartChangeCancel, and CareFirst BlueCross BlueShield is - type in these fields.

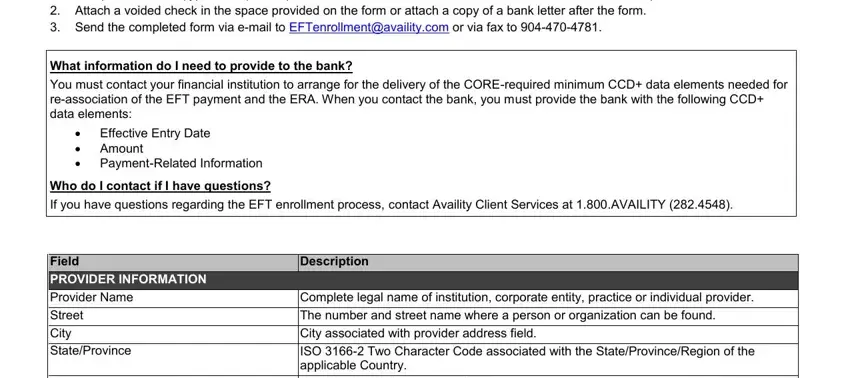
4. The fourth subsection arrives with the following form blanks to type in your specifics in: Complete the form type all, What information do I need to, You must contact your financial, Effective Entry Date Amount, Who do I contact if I have, If you have questions regarding, Field, PROVIDER INFORMATION, Description, Provider Name, Complete legal name of institution, Street, City, StateProvince, and The number and street name where a.
Be very mindful when completing Provider Name and Street, since this is the section where many people make a few mistakes.
Step 3: Just after proofreading the form fields, click "Done" and you're all set! Right after getting afree trial account with us, it will be possible to download carefirst enrollment eft or send it via email immediately. The form will also be at your disposal in your personal account menu with your every single edit. We do not share any information that you use whenever completing forms at our site.