What Is the CareFirst EFT Form?
The CareFirst Electronic Funds Transfer (EFT) Authorization Agreement allows healthcare providers to receive direct deposit payments from CareFirst BlueCross BlueShield. Instead of waiting for paper checks, providers receive ACH credits directly into their bank accounts. This speeds up revenue cycles and reduces administrative overhead.
What Information Does the Form Require?
To complete the authorization, gather the following details before you begin:
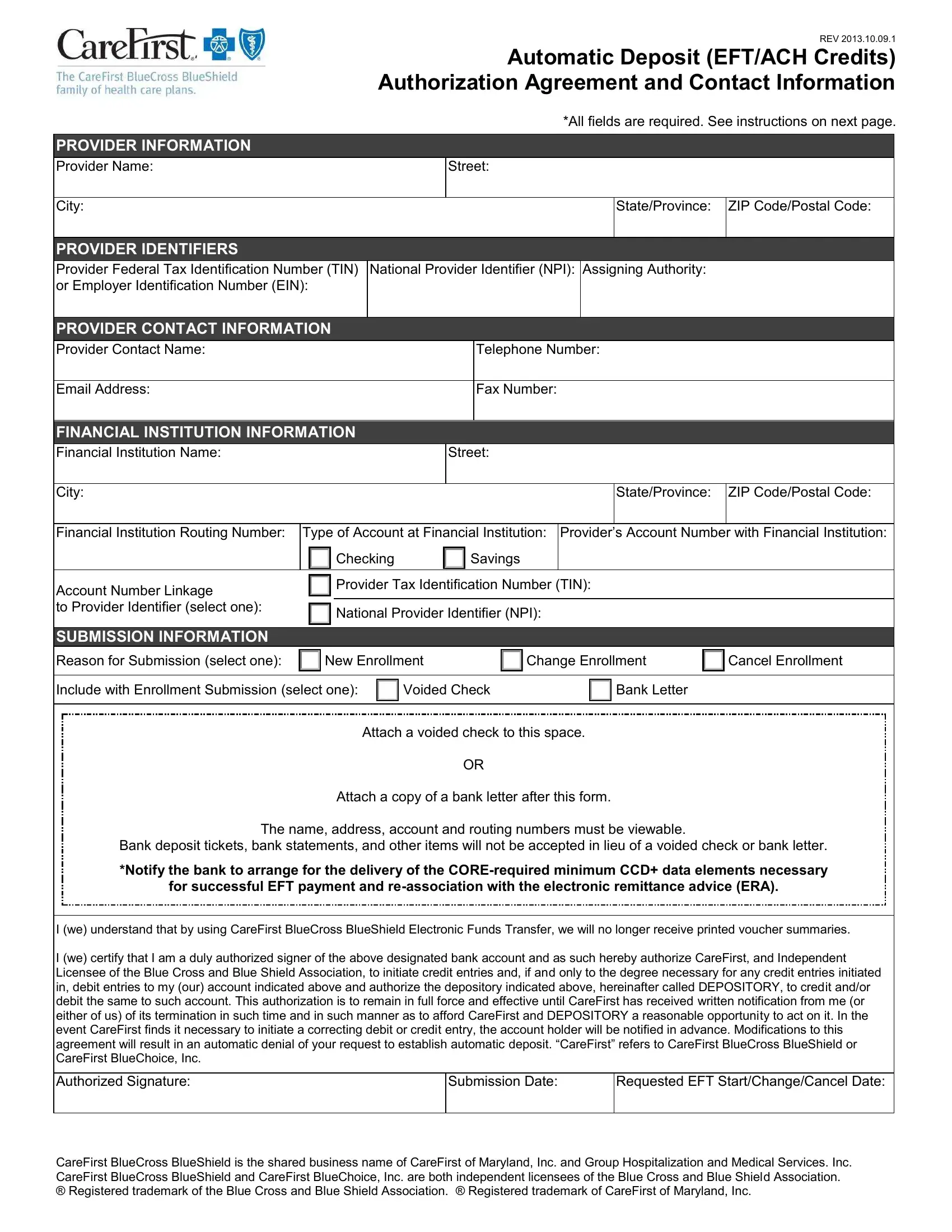
- Provider information: Full legal name and practice address
- Tax ID: Federal Tax Identification Number (TIN)
- NPI: National Provider Identifier
- Banking details: Bank name, routing number (ABA), and account number
- Account type: Checking or savings
- Contact information: Name, title, phone number, and email for EFT inquiries
- Verification documents: A voided check or an official bank letter confirming your account
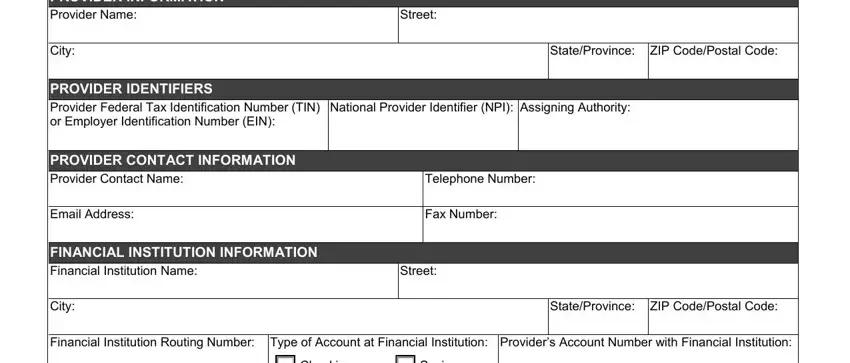
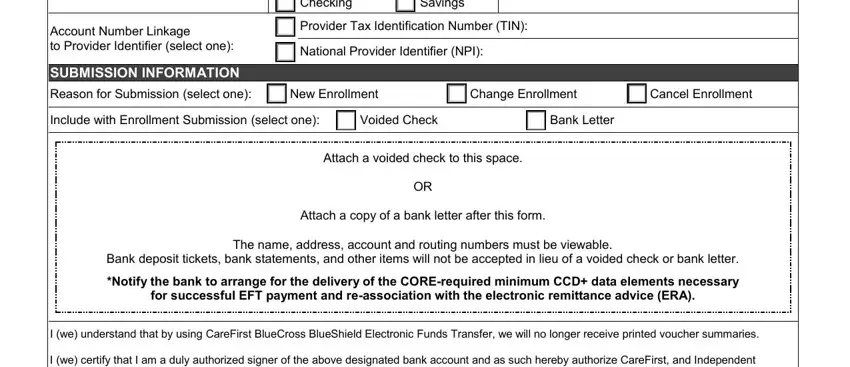
Which Enrollment Option Should You Choose?
The form includes three submission types. Each corresponds to a different change in your EFT arrangement with CareFirst:
- New Enrollment: First-time setup of electronic payments from CareFirst. Use this option if you are not currently receiving direct deposits from CareFirst BlueCross BlueShield.
- Change Enrollment: Updating bank account details, changing the account type, or correcting contact information. You must provide a new voided check or bank letter when changing banking details.
- Cancel Enrollment: Stopping existing EFT deposits and returning to paper check payments. Cancellation is processed within 30 days of receipt.
An authorized representative must sign and date the agreement. The signature confirms that the bank account information is accurate and that the provider agrees to the terms of the arrangement.
Benefits of Setting Up Electronic Fund Transfers
Healthcare providers who switch to direct deposit with CareFirst gain several practical advantages over paper check payments:
- Faster payment cycles — funds arrive days earlier than paper checks
- Reduced risk of lost or stolen checks during mail delivery
- Automatic record-keeping through bank statements and Electronic Remittance Advice (ERA) files
- Lower administrative overhead from manual check processing and deposit runs
- More predictable cash flow for medical practices and healthcare groups
- Easier reconciliation when combined with ERA files — payment and remittance data arrive on the same schedule, reducing manual matching
- Simplified income documentation since bank statements serve as verifiable records of each ACH deposit
- Reduced dependence on physical mail handling and postal schedules for critical revenue
For practices managing multiple payers, EFT consolidates deposits into a predictable channel. This simplifies monthly reconciliation compared to tracking physical check deposits from multiple carriers on different delivery schedules.
In real-world implementations, group practices that switch from paper checks to EFT with CareFirst typically see faster accounts receivable cycles within the first billing period. Case study data from multi-specialty practices shows that automated electronic deposits eliminate the reconciliation time associated with manual check deposits and postal delays.
What Happens After You Submit the Form
Once CareFirst receives your completed EFT authorization, they review the submitted information and verify your banking details. You will receive a confirmation letter or notification when your enrollment is approved and the effective date is set. Processing takes up to 30 days. During this time, CareFirst will continue to issue paper checks for any claims that process before your EFT effective date. After the EFT start date, all eligible claim payments will be deposited directly into your registered bank account.
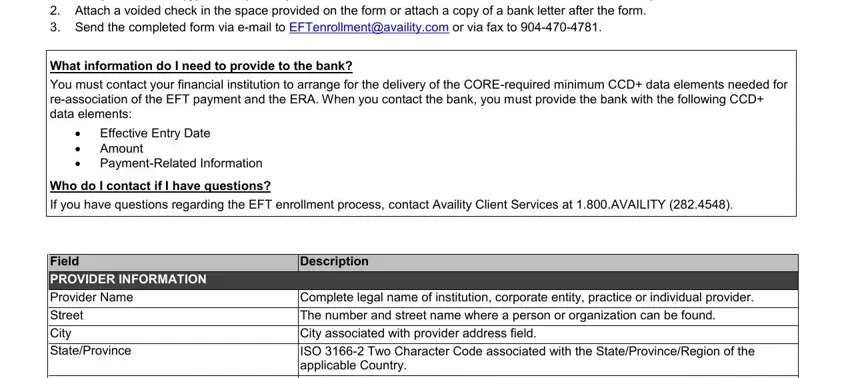
How to Submit the Authorization
After completing the document, attach a voided check or bank letter to verify your account. Submit by mail or fax to CareFirst provider services. Allow at least 30 days for processing before electronic payments begin. Keep a copy of all submitted documents for your records. Providers who submit by fax should retain the fax confirmation page as proof of submission. For current mailing addresses and fax numbers, log in to the CareFirst provider portal or call provider services directly. CareFirst does not accept EFT authorization forms by email or through their online portal — mail and fax are the only accepted submission methods.
Frequently Asked Questions
What is the CareFirst EFT form used for?
It authorizes CareFirst BlueCross BlueShield to deposit claim payments directly into a provider's bank account instead of mailing paper checks. All participating in-network providers can request enrollment.
Who needs to complete this form?
Any healthcare provider contracted with CareFirst who wants to receive electronic payments must submit this authorization document. This includes individual practitioners, group practices, and hospital systems that accept CareFirst BlueCross BlueShield as a payer.
What is the difference between EFT and ACH?
EFT (Electronic Funds Transfer) is the broad category of electronic payments. ACH (Automated Clearing House) is the specific banking network used to process those transfers between financial institutions. The ACH network is governed by NACHA and handles billions of transactions annually across the United States. CareFirst uses the ACH network to execute all EFT payments to providers. Understanding this distinction matters when troubleshooting payment delays — errors in ACH routing or account numbers must be corrected by resubmitting a new EFT authorization with the Change Enrollment option selected.
How long does EFT setup take?
Processing typically takes 30 days from receipt of a completed and correctly filled form. The clock starts when CareFirst receives the form, not when you submit it. Allow extra time for mail delivery if submitting by post rather than fax. If your provider enrollment information changes during the processing period — such as a TIN or NPI update — contact CareFirst before your effective date to confirm whether a new authorization is required.
Can I use this form to update my bank account?
Yes. Select the Change Enrollment option and provide your new banking details along with a new voided check or bank letter. The old account will remain active for incoming deposits until the change is fully processed and confirmed.
What should I do if an EFT payment does not arrive on time?
First verify that your enrollment was processed by contacting CareFirst provider services. Check that the enrollment effective date has already passed — payments issued before your EFT effective date will still arrive as paper checks even if your enrollment is active. Confirm your bank routing number and account number are correct on file. If an error exists in the registered details, resubmit the authorization with the accurate banking information and a new voided check. If a payment is delayed beyond the expected posting window, contact your bank to verify no ACH credit holds or returns occurred on the account.
Is there a fee for enrolling in EFT with CareFirst?
No. CareFirst does not charge providers a fee to enroll in electronic funds transfer. The service is provided as part of CareFirst's standard provider payment process. Your bank may have its own policies for receiving ACH credits, so check with your financial institution if you have questions about your account.
What documents do I need to attach to the form?
You must attach either a voided check or an official letter from your financial institution on bank letterhead. The document must show the bank name, routing number, and account number for the account where you want deposits sent. Make sure the attached document is for the same account listed on the authorization form.
Can a group practice enroll multiple providers under one bank account?
Yes. Group practices and health systems can route payments for multiple providers into a single bank account, provided the account is registered under the same Tax Identification Number used on the authorization form. Each individual provider in the group must be identified by their own National Provider Identifier. Large group practices enrolling several providers at once should contact CareFirst provider services for guidance on coordinating the authorization process and expected processing timelines for each provider.
Do I need to enroll separately if I already receive EFT from another insurer?
Yes. Each health insurer manages its own electronic payment enrollment independently. An existing EFT arrangement with Medicare, Medicaid, or another commercial payer does not extend to CareFirst BlueCross BlueShield. You must complete and submit this CareFirst-specific EFT authorization to begin receiving direct deposits from CareFirst, even if you already receive electronic payments from other carriers using the same bank account.
Does EFT enrollment with CareFirst also include Electronic Remittance Advice setup?
No. Electronic Remittance Advice (ERA) is a separate enrollment process from EFT. ERA delivers a detailed electronic explanation of benefits alongside each claim payment. Many providers enroll in both EFT and ERA at the same time to automate payment posting in their practice management system. ERA enrollment is typically handled through your clearinghouse or billing service, or through the CAQH ProView provider enrollment portal — confirm with your billing team about the ERA setup process after completing EFT enrollment with CareFirst.
Can I cancel my EFT enrollment and re-enroll later with updated banking information?
Yes. Use the Cancel Enrollment option to stop direct deposits and return to paper check payments. You can re-enroll at any time by submitting a new authorization with the New Enrollment option selected. Each change or new enrollment request takes up to 30 days to process. If you are switching banks, wait until your cancellation is confirmed before submitting a new enrollment to avoid payment overlap or deposit errors during the transition period.
Will I still receive paper checks after enrolling in EFT?
Yes, during the transition period. After submitting the authorization, CareFirst will continue issuing paper checks for any claims that process before your EFT effective date is confirmed. Once the effective date passes, all eligible claim payments shift to direct deposit. Some claims may still result in paper checks if they involve secondary payers or other billing circumstances outside the EFT arrangement. Contact CareFirst provider services if paper checks continue arriving more than 30 days after your confirmed EFT effective date.
FormsPal also provides a general electronic funds transfer form, a CareFirst cancellation form, and a CAQH provider enrollment application.
| Question | Answer |
|---|
| Form Name | Carefirst Eft Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | carefirst eft enrollment, carefirst deposit eft ach, carefirst eft change, automatic deposit eft ach carefirst |