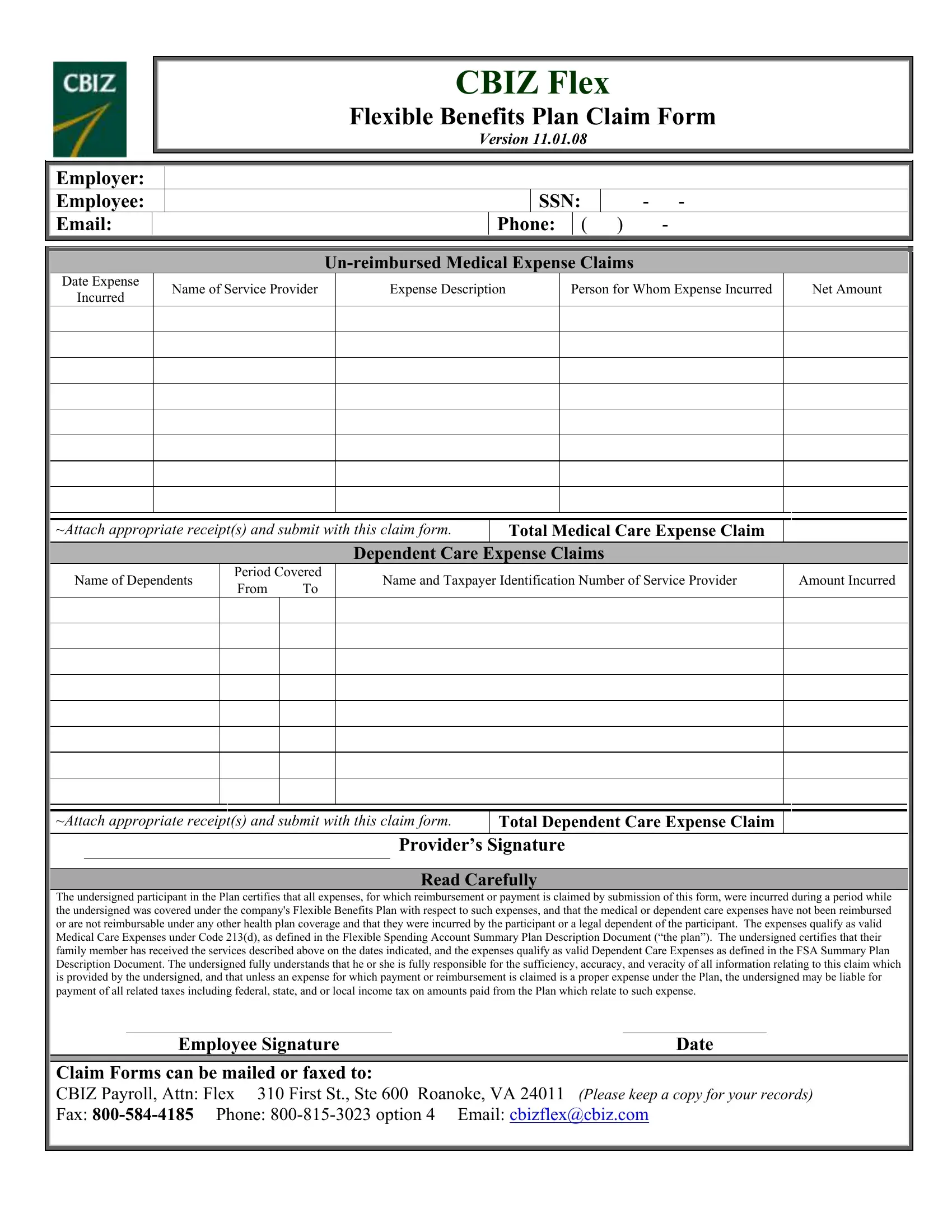
Understanding the CBIZ Flex Flexible Benefits Plan claim form is pivotal for employees who seek reimbursement or payment for medical or dependent care expenses that were incurred while covered under their company's Flexible Benefits Plan. This comprehensive form requires detailed information, including the employer and employee particulars, Social Security Number, contact information, and specifics about the un-reimbursed medical or dependent care expenses. It mandates the inclusion of the date the expense was incurred, the service provider's name, a brief description of the expense, who the expense was for, and the net amount, all supported by the necessary receipts. A separate section is dedicated to dependent care expense claims, capturing the name of the dependents, period covered, service provider details, and the amount incurred. Further cementing its importance is the certification section, where the employee attests that the expenses listed are not reimbursable under any other health plan, were incurred legitimately as per the plan's guidelines, and acknowledges their responsibility for the accuracy of the information provided. The form also outlines how it should be submitted for processing, reinforcing the significance of keeping a copy for personal records. This vital document bridges the gap between incurring medical or dependent care expenses and receiving the appropriate benefits under the Flexible Spending Account (FSA), crucial for managing personal finances effectively.
| Question | Answer |
|---|---|
| Form Name | Cbiz Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | cbiz flex online, cbiz flex plan, cbiz flex claim form, cbiz claim form |
CBIZ Flex
Flexible Benefits Plan Claim Form
Employer:
Employee:
Email:
VERSION 11.01.08
|
SSN: |
|
- - |
||
|
|
|
|
|
|
Phone: |
|
( ) |
- |
||
Date Expense
Incurred
Name of Service Provider
Expense Description
Person for Whom Expense Incurred
Net Amount
~Attach appropriate receipt(s) and submit with this claim form.
Total Medical Care Expense Claim
Dependent Care Expense Claims
Name of Dependents
Period Covered From To
Name and Taxpayer Identification Number of Service Provider
Amount Incurred
~Attach appropriate receipt(s) and submit with this claim form.
Total Dependent Care Expense Claim
Provider’s Signature
Read Carefully
The undersigned participant in the Plan certifies that all expenses, for which reimbursement or payment is claimed by submission of this form, were incurred during a period while the undersigned was covered under the company's Flexible Benefits Plan with respect to such expenses, and that the medical or dependent care expenses have not been reimbursed or are not reimbursable under any other health plan coverage and that they were incurred by the participant or a legal dependent of the participant. The expenses qualify as valid Medical Care Expenses under Code 213(d), as defined in the Flexible Spending Account Summary Plan Description Document (“the plan”). The undersigned certifies that their family member has received the services described above on the dates indicated, and the expenses qualify as valid Dependent Care Expenses as defined in the FSA Summary Plan Description Document. The undersigned fully understands that he or she is fully responsible for the sufficiency, accuracy, and veracity of all information relating to this claim which is provided by the undersigned, and that unless an expense for which payment or reimbursement is claimed is a proper expense under the Plan, the undersigned may be liable for payment of all related taxes including federal, state, and or local income tax on amounts paid from the Plan which relate to such expense.
Employee SignatureDate
Claim Forms can be mailed or faxed to:
CBIZ Payroll, Attn: Flex 310 First St., Ste 600 Roanoke, VA 24011 (Please keep a copy for your records)
Fax: