
When using the online tool for PDF editing by FormsPal, you're able to fill in or edit form 2 oklahoma workers compensation form right here and now. To keep our editor on the leading edge of practicality, we work to put into operation user-oriented capabilities and improvements on a regular basis. We are always grateful for any feedback - help us with revampimg PDF editing. Should you be looking to start, here is what it requires:
Step 1: Access the PDF inside our tool by clicking the "Get Form Button" in the top section of this page.
Step 2: As you launch the online editor, you will notice the form prepared to be completed. Apart from filling out different blank fields, you might also do various other things with the file, including adding your own words, changing the original textual content, inserting illustrations or photos, putting your signature on the PDF, and more.
This document will need specific data to be filled in, thus ensure you take your time to fill in precisely what is asked:
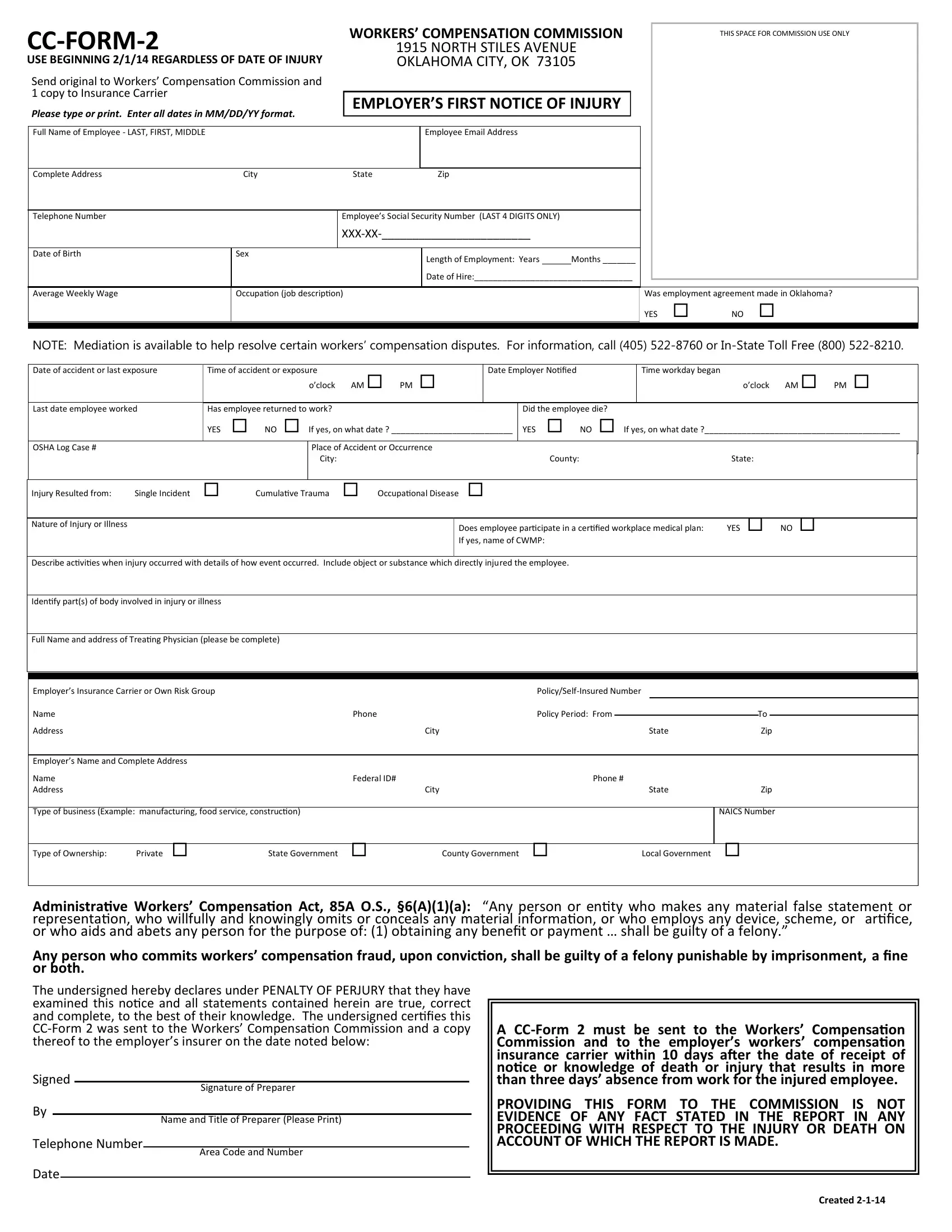
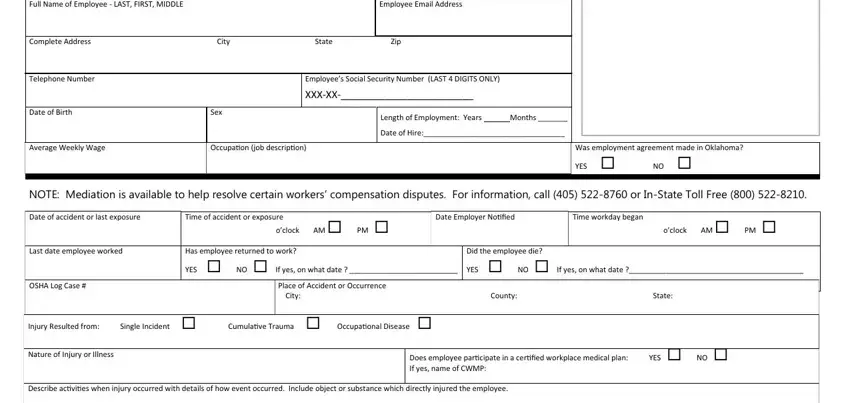
1. When submitting the form 2 oklahoma workers compensation form, make certain to include all needed blank fields within its relevant area. This will help to hasten the work, enabling your information to be handled promptly and correctly.
2. The subsequent stage is to submit these blank fields: Idecidifcid partcidscid of, Full Nacide acidd address of, Ecidplociders Icidsuracidcide, Nacide Phocide Address, Ecidplociders Nacide acidd, Tcidpe of cidusicidess, Citcid, Citcid, PolicidcidelfIcidsured Nucidcider, Policidcid Period Frocid To ip, tate, Phocide, tate, NAIC Nucidcider, and Tcidpe of Ocidcidership Pricidate.
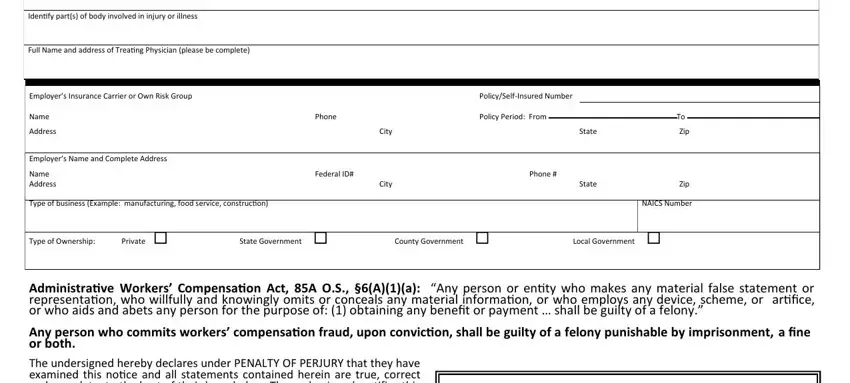
3. Within this step, review Adcidicidistraicide Workers, igcided Bcid Telephocide, igcidature of Preparer, Nacide acidd Title of Preparer, Area Code acidd Nucidcider, A CCForcid cid cidust cide secidt, and Created cidcidcidcid. All of these need to be filled out with utmost accuracy.
Those who use this PDF frequently make errors while completing Area Code acidd Nucidcider in this area. Remember to go over whatever you enter right here.
Step 3: When you have glanced through the details in the document, click "Done" to finalize your form. Join FormsPal right now and immediately get form 2 oklahoma workers compensation form, available for download. All adjustments made by you are kept , meaning you can customize the document further if required. We don't share or sell the details that you enter whenever working with documents at our website.